Neurodermatitis
It is a recurrent disease that manifests itself with two main symptoms: inflammation and itching of the skin. This is a chronic disease that can appear in childhood and accompany you throughout your life. Life for people with neurodermatitis is very difficult due to the frequent manifestation of symptoms. When fighting this disease, the main task is to maximize the periods of calm skin.
The exact causes of the disease have not been established, but it is generally accepted that it is caused by genetic factors and characteristics of the skin. There are factors that most often provoke the manifestation or exacerbation of neurodermatitis (we will talk about them in our article).
Nowadays, the term “neurodermatitis” is a replacement for the term atopic dermatitis. Conducted studies have shown that the impetus for the development of the disease is stress or a viral infection (in adults). The vast majority of patients learned about their diagnosis when symptoms appeared in childhood (up to 7 years). In childhood, manifestations are provoked by allergies.
Symptoms
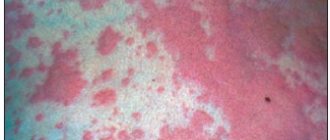
Neurodermatitis has pronounced symptoms, namely: severe itching, flaking of the skin, redness (on the elbows and knees and skin folds on the neck). In addition, purulent formations and rashes may form on the face. Sometimes the disease is combined with other diseases, such as asthma, allergic rhinitis, pollionosis.
Factors influencing the exacerbation of neurodermatitis:
- • Constant contact with possible allergens: dust, animal hair, pollen, food allergens;
- • Stress, strong emotional shocks;
- • Malfunctions of the hormonal system;
- • Gastrointestinal problems;
- • Incorrect use of medications;
- • Failure to comply with hygiene rules.
* Atopic dermatitis is associated with heredity, so if one or both parents have this disease, it is highly likely to be passed on to the unborn child.
Manifestations of the disease at various stages.
Usually the very first manifestations of neurodermatitis are noticeable in the first months of life. They appear in the form of flaky redness of the skin on the face (around the eyes, behind the ears, in the eyebrow area, on the cheeks). As the child grows up, the location of the redness may change (mucous membranes of the eyes, nose, genitals. Exacerbations most often occur in the autumn-winter period, and in the summer the condition improves. The most noticeable symptom is severe itching! It is pathological in nature. When scratching, micro- wounds through which infection can get in. That is why the symptoms of neurodermatitis should be dealt with.
Sometimes (during remission) symptoms improve or disappear completely. This period can last from several weeks to several years. If the symptoms of neurodermatitis have not bothered you for more than 7 years, then we can talk about your recovery. However, since the disease has not been fully studied, there is no clear understanding of whether the disease is gone forever. There is a possibility of her return.
Atopic dermatitis and mental disorders: psychosomatic relationships
Atopic dermatitis (AD) is a hereditary, immunoneuroallergic, chronic recurrent inflammatory skin disease caused by atopy, manifested by intense itching, sympathetic skin reaction (white dermographism), predominantly erythematous-lichenoid rashes, in combination with other signs of atopy.
In 1923, American allergists Coca AF and Cooke RA, wanting to describe an unusual type of hypersensitivity to various environmental substances, which occurred only in humans and was more common in families without obvious previous sensitization, turned to philologist Perry from Columbia University for help. He suggested that scientists use the term “atopy,” which means “out of place” or “strange” [29]. Atopy is understood as a hereditary predisposition to allergic reactions in response to certain antigens. The first “atopic” described in the literature was Emperor Octavius Augustus, who was described as having extremely severe itching, seasonal rhinitis and shortness of breath. In addition, his family history is described in detail: his grandson, Emperor Claudius, suffered from symptoms of rhinoconjunctivitis, and his great-nephew, Britannicus, suffered from an allergy to horse epithelium [41]. For more than 80 years, the term “atopy” has been used throughout the world, although it is sometimes the subject of debate.
AD is an extremely common and often severe dermatosis. Its frequency in the structure of skin diseases, according to various sources, ranges from 20 to 40%. Epidemiological studies show that AD is more common among young people than adults. Both sexes are affected, slightly more often women. AD occurs in people all over the world and in all races. Over the past decades, the prevalence of the disease has increased significantly. For example, in Denmark, the overall incidence of twins under 7 years of age born from 1960 to 1964 was 3%. And for twins born from 1970 to 1974, this figure has already increased to 10% [44].
The occurrence and chronic course of AD is determined by hereditary predisposition, functional disorders of the nervous system, the influence of unfavorable environmental conditions, psycho-emotional disorders and pathology of internal organs, metabolic, neurohumoral, neurovascular disorders, allergic diseases, poor nutrition, and various intoxications [14].
The clinical manifestations of AD are varied, but quite typical and well studied. The disease usually begins in early childhood, most often in the second half of life. It can last for many years, characterized by remissions, mainly in the summer, and relapses in the spring and autumn periods of the year. Over time, the severity of the disease weakens, and at the age of 30–40 years, spontaneous recovery occurs in most patients. During the course of the disease, three phases are distinguished: infant (usually from 7–8 weeks of life to 3 years), childhood (from 3 to 7 years) and adult. In the infant and childhood phases, focal erythematous-squamous rashes with a tendency to exudate (vesiculation, weeping) on the skin of the face, buttocks, and extremities are more often observed. In the adult phase, itchy erythematous-lichenoid rashes predominate on the flexor surfaces of the extremities and on the neck with the development of lichenization (the skin becomes thickened, rough to the touch, the skin pattern is pronounced). The degree of severity and prevalence of the process can be different - from limited (perioral) rashes to extensive damage to the skin like erythroderma. An indispensable sign of AD, regardless of the phase of its course or clinical variant, is intense itching, which forms the basis of the patient’s suffering, significantly aggravating the course of the disease and reducing the quality of life [6, 15, 42].
In accordance with the clinical classification of Sergeev Yu.V. [14], there are five forms of AD: lichenoid, erythematous-squamous, pruriginous form, eczematous, atypical.
The diagnosis of AD is based on a set of diagnostic signs of AD, which is called the Hanifin A criteria. Rajka, 1980 (
) [37]. The diagnosis of AD requires the presence of at least three of the four major criteria and three minor criteria.
To objectively assess the severity and extent of the skin process and the severity of itching in AD, a group of researchers from the European Center for the Study of AD developed a unified symptom scale (SCORAD), which is a multiparameter score for the severity of AD, which can be used as the most objective (“golden”) ”) standard in scientific research and clinical practice [32].
As a disease whose exacerbations can be provoked psychogenically, AD was classified as a classical psychosomatic disease by Franz Alexander in 1950 [21]. Since then, a large number of domestic [3, 4, 5, 8, 9, 10, 11, 12, 13, 18] and foreign [19, 20, 37, 22, 23, 28, 30, 33] studies have been conducted, dedicated to studying the role of psychogenic influences as factors provoking exacerbation of blood pressure, as well as mental disorders in patients with blood pressure. Using the AD model, it seems possible to study mental disorders that develop in patients with chronic pruritic dermatoses. It is believed that the localization of rashes on visible areas of the skin and severe itching lead not only to a decrease in the quality of life, but also to the development of pathological mental reactions to the disease, which significantly affect the patient’s compliance during therapy and further aggravate the condition of patients.
According to studies, blood pressure often worsens after psychogenic influences and is often accompanied by mental disorders [24, 25, 26, 27, 34, 35, 38, 39]. Thus, the association of blood pressure and depressive disorders was established in studies of the comorbidity of the discussed dermatosis and affective pathology. According to a cohort study conducted by Timonen M., 30% of patients with AD experience episodes of depression during their lifetime [45], which significantly exceeds this figure in the general population (from 5% to 10%) [43]. In studies by other authors, depression was detected in 23–80% of patients with AD [1, 5, 11, 12, 13, 18]. Comorbidity of anxiety disorders and blood pressure was observed in almost half of the patients studied [4, 46]. There is evidence that the psychological profile of “atopic” is characterized by depression, tension, anxiety and aggressiveness [25, 28, 33]. In this case, the frequent development of mental disorders is explained, as a rule, by the nature of the skin disease (chronic course, intense, including nighttime, itching and localization of rashes on visible areas of the skin).
However, the conducted psychosomatic studies of patients with AD are mostly based either on the use of formalized psychometric diagnostic methods or psychological counseling and do not allow assessing the proportion of truly nosogenic mental deviations and the proportion of disorders that developed regardless of AD.
In recent years, a taxonomy of psychodermatological disorders has been created (
). According to this classification, AD belongs, on the one hand, to the group of psychosomatic diseases, on the other hand, chronic dermatosis can be the cause of the development of nosogenic reactions and pathological developments. However, there have been no studies of the characteristics of mental disorders in AD from these positions.
The purpose of this study was a comprehensive clinical study of mental disorders in AD and their connection with the clinical features and course of the skin disease, aimed at developing their typological differentiation.
Material and research methods
The study material consisted of 97 patients (73 women and 23 men; average age 26.9 ± 10.2 years).
Inclusion criteria: verified diagnosis of AD according to the international diagnostic criteria of JM Hanifin and G. Rajka [37], patient age from 18 to 65 years.
Exclusion criteria: manifest schizophrenic/schizoaffective/affective psychosis, organic damage to the central nervous system, dementia, addiction to psychoactive substances, other severe somatic diseases in the stage of exacerbation or decompensation.
The study was conducted using a clinical method, which included a comprehensive dermatological and psychopathological examination. Dermatological examination included analysis of anamnestic and clinical indicators, confirmation of the diagnosis of AD. The severity and extent of the skin process in all patients were assessed using the SCORAD index (method recommended by the European Working Group on AD [32], which takes into account the prevalence of rashes, the nature of the rash (erythema, edema, oozing, excoriation, lichenification, dryness) and the severity of subjective symptoms - itching, blood pressure-related insomnia.
The psychopathological examination was carried out by employees of the department for the study of borderline mental pathology and psychosomatic disorders (headed by Academician of the Russian Academy of Medical Sciences A. B. Smulevich) of the National Center for Mental Health of the Russian Academy of Medical Sciences, the Department of Psychiatry and Psychosomatics of the Faculty of Physical Education of the Moscow Medical Academy named after. I. M. Sechenova, Ph.D. Dorozhenkom I. Yu., Ph.D. M. A. Terentyeva, Ph.D. V. I. Frolova, K. A. Baturin. An experimental psychological examination was carried out by O. V. Petukhova, D. A. Beskova, L. T. Kozlovskaya. The final qualification of psychopathological disorders was carried out by Academician of the Russian Academy of Medical Sciences A. B. Smulevich as part of clinical reviews, to which all patients were presented.
results
Dermatological examination revealed that the average duration of the disease was 19.99 ± 12.04 years.
According to the severity, the patients were distributed as follows: mild AD was diagnosed in 37 patients (38.1%), moderate AD in 30 patients (31%), severe AD in 19 subjects (19.6%), and very severe AD. in 11 patients (11.3%).
The studied sample included patients with different forms of AD: 72 (74.2%) patients were diagnosed with erythematous-squamous form of AD, 17 (17.5%) - eczematous, 7 (7.2%) - lichenoid, 1 (1.1%) - prurigo-like. Among them, 37 patients (38.1%) at the time of examination had a skin disease in the chronic stage and 60 (61.9%) had an exacerbation of blood pressure.
During a psychopathological examination, a number of mental disorders were identified in 52 patients (53.6%), which were not only caused by the influence of dermatological pathology (nosogenic reactions and personality development), but also developed without a direct connection with blood pressure. The examination revealed a wide range of mental disorders, which include nosogenic reactions, hypochondriacal pathocharacterological developments, affective disorders and low-grade schizophrenia (
; Some patients had several mental disorders at the same time).
Anticipating the clinical characteristics of nosogenic reactions, it should be noted that their manifestation in patients with AD is determined not only by the course of the skin disease (the development of exacerbations often without a reason obvious to the patient, the localization of rashes on visible areas of the skin) and the existing ideas among the population about the contagiousness of skin diseases, but also constitutional abnormalities (personality disorders (PD)), responsible for the predisposition to the formation of pathological reactions and significantly influencing the symptoms and dynamics of nosogenies:
1. In the formation of sensitive nosogenic reactions (n = 12, 12.4%), the phenomena of social phobia associated with a cosmetic defect caused by AD dominate, while physical discomfort associated with a skin disease is perceived by patients as a significantly less relevant manifestation of AD. Social phobia is represented by fear of the negative attitude of others, mainly dissatisfaction and alienation for fear of infection, due to changes in the skin on visible parts of the body. Pathological fears are accompanied by fragmentary, unsystematized and not reaching the delusional level of ideas of attitude: it seems to patients that those around them (on the street, in transport) look especially sympathetically or condemningly, as if they were looking at a sick person, deliberately distance themselves or move away, fearing infection, whispering indignantly discuss among themselves, expressing dissatisfaction with the presence of the patient, etc. In accordance with the plot of dominant fears, pathological avoidant behavior is formed: before going out in public, patients carefully mask skin rashes with cosmetics, choose the most revealing clothes, and often completely refuse to visit crowded places.
Premorbid characteristics of patients with this type of nosogenies, regardless of the age of manifestation of AD, are represented by schizoid and hysterical PD.
When assessing the demographic characteristics of the clinical picture, one should first of all note the average age, which in the group of sensitive reactions was 23.3 ± 12.7 years, which is 3 years less than the average for the sample. The second distinguishing characteristic of this group of patients was the SCORAD score, which was 34 ± 3.5, which is less than the average for the overall study sample (40.5 ± 7.07). According to the dermatological examination, in the group of sensitive nosogenic reactions, the predominance of the erythematous-squamous form of AD was established, which is the dominant form of AD in the entire studied sample (only one patient had an eczematous form). The data presented indicate that the development of sensitive nosogenic reactions is typical for young patients with a relatively mild severity of AD.
2. Anxiety-hypochondriacal nosogenic reactions (n = 16, 16.5%) developed at the onset of AD in adult patients after a long-term complete clinical remission observed since childhood. Signs of nosophobia came to the fore, represented by the fear of chronic disease, the possibility of damage to internal organs, the need for constant hospital treatment, etc. Pursuing the goal of complete cure of AD, patients resorted to repeated visits and hospitalizations, sought to conduct all kinds of available examinations to identify the main cause of AD and carrying out appropriate therapy, studied the available literature on the diagnosis and treatment of AD.
Premorbid personality characteristics involved in the formation of the type of nosogenic reactions under consideration are represented by constitutional anomalies of the anxiety circle, mainly within the framework of anancastic personality disorder, and schizoid PD.
Analysis of dermatological examination data showed that a distinctive feature of AD in patients with anxiety-hypochondriacal nosogenic reactions is, firstly, its average duration, which turned out to be the shortest compared to other nosogenic reactions (7 ± 5.3), and, secondly, , the severity of AD according to SCORAD, which was the greatest (54 ± 19.1), in contrast to other nosogenic reactions. It should be noted that such indicators of the clinical dynamics of somatic pathology - rapid progression and severe levels of symptoms - are traditionally considered among the factors contributing to the formation of alarming nosogenic reactions. In addition, the average age of patients with this type of reaction was 34 ± 5.1 years, which is greater than that of patients with AD with sensitive nosogenic reactions.
Summarizing the features of AD in the group of patients with various nosogenic reactions, it can be noted that the course of AD was characterized, as a rule, by regression of rashes at the end of the infant phase of AD, followed by complete or almost complete clinical remission and resumption of the rash in adolescence in the form of exacerbations of AD that caused reactions within the dynamics of personality disorders. Sensitive reactions were noted in younger patients (23.3 ± 3.1), in contrast to the anxious-hypochondriacal reactions detected in older patients (34 ± 5.1). The average SCORAD score was lowest in patients with sensitive nosogenic reactions (34) and highest in patients with anxiety-hypochondriacal nosogenic reactions (47). Thus, the development of certain nosogenic reactions may be associated with age, severity, duration of existence of AD, but not with its clinical form.
In cases of prolonged course of exacerbations of AD with frequent relapses and an almost complete absence of periods of complete clinical remissions, deeper and more persistent signs of the dynamics of premorbid personality properties, qualified within the framework of hypochondriacal developments (ID), were revealed. As a result of clinical analysis, 4 types of IR in AD were identified: paranoid, aberrant hypochondria type, masked hypochondria type and neurotic hypochondria type.
1. Paranoid IR [2] (n = 3) is represented by ideas of invention associated with the belief in the possibility of an independent complete cure of a skin disease. Patients resort to developing their own paramedical treatment methods, sometimes accompanied by autodestructive (harmful or hazardous to health) actions (ingestion of crushed stones, metal powders made independently).
A similar type of development is formed in patients with PD of the paranoid circle (a tendency to form overvalued ideas combined with suspicion and distrust towards others, which are often deliberately perceived as potential sources of threat to the realization of one’s own aspirations).
The manifestation of the skin disease in these patients was observed at the age of 20–25 years and was characterized by a severe course. All patients with paranoid personality development exhibited widespread AD (erythematous-squamous form, n = 2) or erythroderma with severe dryness and peeling of the skin, which was accompanied by low-grade body temperature and lymphadenopathy (n = 1). In one case, the development of AD was provoked psychogenically (after the patient lost her job).
2. Development according to the type of aberrant hypochondria [31] (n = 6) is characterized by an underestimation of the severity of the condition (lack of emotional reaction to the threatening meaning of the diagnosis) with a desire to minimize ideas about the possibility of a severe course of somatic illness. Manifestations of skin pathology are interpreted as only minor deviations from the norm. In some cases, the type of IR in question is accompanied by maladaptive behavior, which often interferes with medical care and treatment procedures. The dermatological status of this group of patients was characterized by mild and moderate severity of AD, mainly localized in closed areas of the skin. Premorbid features of patients with this type of development are represented by accentuation of the type of segmental depersonalization [40], acting within the framework of hyperthymic RL.
3. Development according to the type of masked hypochondria [40] (n = 17) is manifested in a structured gradual adaptation to the manifestations of the disease as a habitual, inevitable companion and an obligatory component of everyday life. With the phenomena of masked hypochondria, patients establish a “partnership” relationship with the disease, on the one hand, following medical recommendations with regular implementation of the necessary therapeutic and preventive measures, on the other hand, continuing to lead an active lifestyle, without “discounts” on their health status. IR of the type of masked hypochondria is formed in individuals with accentuation of the type of proprioceptive diathesis.
The following features of the course of the dermatological disease were noted. AD either 1) manifested in early childhood and the rash persisted throughout life, while the severity and course could be very different, ranging from isolated episodic recurrent erythematous-squamous rashes to widespread lichenoid lesions reaching the level of erythroderma, which within have not undergone complete clinical remission for many years; 2) or the development of this dermatosis was noted after 15–20 years, but the disease was mild (limited rashes that occur only occasionally and necessarily completely regress in the warm season).
4. Development according to the type of neurotic hypochondria [36] (n = 7) occurs with a predominance in the clinical picture of manifestations of somatized anxiety and an increase in real symptoms of AD due to somatoform disorders (the appearance of itching as part of a somatoform disorder with a subsequent increase in scratching and provocation of the appearance of new rashes) . Patients show a clear tendency to create a gentle lifestyle for themselves (a protective regime with a significant limitation of stress, both domestic and work), and any attempts by medical personnel and relatives to activate the patient are met with accusations of insensitivity and insufficient understanding of the severity of the disease. Development of the type of neurotic hypochondria is detected in individuals with a neuropathic constitution within the framework of schizoid PD.
This type of development was observed mainly in patients with mild and moderate AD, which responds well to conventional therapy, but often affects exposed areas of the skin.
In patients with affective disorders identified during the examination, seasonal depression was more often detected (35.3% of all patients with depression) (
). Psychogenically provoked depression was in second place in terms of prevalence (29.4% of cases). Endogenous depression was detected somewhat less frequently (17.6% of patients with depression). Nosogenic depression was diagnosed in only 11.6% of patients and ranked only fourth in prevalence in the studied sample. Postpartum depression was identified in 5.9% of atopic patients with depression.
When analyzing dermatological status, it was found that the average SCORAD scores in patients with depression at the time of examination (46.4) were slightly higher than in patients who had not had a single episode of mood disorders during their lifetime (38.1), and higher than the average SCORAD score in the entire study sample (40.6). These differences, however, did not reach the level of statistical significance, which is apparently explained by the small number of patients with depression in the examined sample.
In the group of patients with depression, rashes were more often localized on the face (
), which is consistent with literature data [7, 17].
It was also found that the highest subjective assessment of the intensity of itching according to SCORAD (10 points) is characteristic of patients with nosogenic depression.
When comparing the frequency of recurrence of AD in a group of patients suffering from depression with a group of patients without affective disorders throughout life, it was found that the development of depression did not depend on the frequency of recurrence of the skin disease. Thus, in the group of patients with depression, there were an average of 10.6 relapses per patient during life, and in the group of patients without episodes of affective disorders in history or during examination, there were an average of 11.2 exacerbations of blood pressure per patient.
The average duration of blood pressure in patients with low-grade schizophrenia (19.3 years) did not differ significantly from that in patients without this mental illness (20.1 years). The average number of AD relapses experienced in patients with VS (17.1) also did not differ significantly from that in other patients (15.2).
However, the average SCORAD score in patients diagnosed with low-grade schizophrenia was lower than in the other patients examined (36.6 versus 40.9 points). In ten examined patients (81%) the erythematous-squamous form of AD was diagnosed, and in only one case - eczematous (9%).
As a comparison of the therapeutic and control groups showed, the prescription of complex psychopharmacotherapy not only leads to a reduction in psychopathological symptoms compared to the control group, but also promotes a more rapid regression of rashes and itching - the main manifestations of atopic dermatitis. The following drugs have been effective in treating the above disorders.
In the presence of psychopathic personality reactions, it is advisable to prescribe benzodiazepine anxiolytics (Phenazepam 1 mg n/a, Lorazepam 2.5 mg n/a), and if they are intolerant, the mercaptobenzimidazole derivative Afobazole (30 mg/day course for 6 weeks) or the drug hydroxyzine Atarax hydrochloride (12.5 mg morning and afternoon, 25 mg at night).
When paranoid hypochondriacal personality development and neurotic hypochondriasis are identified, their correction is possible with the prescription of atypical antipsychotics, which also show affinity for co-anesthesiapathic disorders of the hypochondriacal spectrum: sulpiride, quetiapine.
For the treatment of affective disorders represented by various depressions (seasonal, psychogenic, endogenous, nosogenic), the administration of fluvoxamine (Fevarin) is effective according to the following scheme: the starting dose of the drug is 50 mg (1-2 days), then it is increased to 100 mg (3 –5th day); starting from the 6th day of therapy, the dose is titrated individually within the range of 100–300 mg/day. The average daily dose of Fevarin is 200 mg/day.
To treat the symptoms of low-grade schizophrenia, the antipsychotic drug Rispolept (risperidone) can be used. The initial dose of the drug is 2 mg/day, on days 2–3 the dose is increased to 4 mg/day.
Thus, the study confirmed the data of previous studies on the high prevalence of mental disorders in patients with AD, identified in 53.6% of patients. As a result of a psychopathological examination, a wide range of comorbid AD mental pathology was established, represented by nosogenic reactions, hypochondriacal personality development, affective disorders and sluggish schizophrenia. It was found that mental disorders in patients with AD are not only associated with a decrease in the quality of life of patients, but also lead to a significant decrease in patient compliance with conventional dermatotropic therapy. The data obtained indicate the need for adequate psychiatric care for this group of patients. Carrying out effective treatment of mental disorders comorbid with AD requires a differentiated approach taking into account the clinical typology of psychopathological disorders.
For questions regarding literature, please contact the editor.
A. N. Lvov , Doctor of Medical Sciences, Professor S. V. Ivanov , Doctor of Medical Sciences, Professor A. V. Michenko , Candidate of Medical Sciences MMA named after. I. M. Sechenova, Moscow
Key words: atopic dermatitis, chronic pruritic dermatoses, depression, tension, anxiety and aggressiveness, taxonomy of psychodermatological disorders, quality of life of patients.
Diagnosis of neurodermatitis.
If symptoms occur, you should contact a dermatologist for a diagnosis. If at least 3 of the listed factors are present, the doctor will suspect neurodermatitis:
- • Skin itching;
- • Visibility of skin lesions;
- • Hereditary factor;
- • Presence of relapses;
- • Exacerbations due to allergies or severe stress;
- • Frequent skin infections;
- • Dark circles around the eyes;
- • Exacerbations in the autumn-winter period;
- • Dry skin;
- • The appearance of additional folds on the lower eyelids.
* After studying the factors, the diagnosis is confirmed or refuted by laboratory tests. A general and biochemical analysis of blood, urine and feces, as well as allergy tests are prescribed.