From this article you will learn:
- how effective is retinol for the face,
- what forms of retinol are there,
- effective concentrations, timing of application.
The article was written by a specialist with higher medical education.
Retinol is one of the most effective ingredients in anti-aging cosmetics, which helps even out skin tone and texture, increase skin elasticity, and reduce the appearance of fine lines and wrinkles. Retinol is just one of many forms of vitamin A, which also include retinoic acid and retinaldehyde, as well as the so-called retinol esters (for example, retinol palmitate or retinol acetate).
Below you will see that real pure retinol and retinol esters are completely different in effectiveness forms of vitamin A. And it is preferable that retinol for facial skin be present in cosmetic products in the form of pure retinol, and not its esters. And below we will tell you why this is so important and how it affects the effectiveness of correcting age-related skin changes.
The best companies producing retinol products are:
The author of this article has a medical education and problem skin, so I know from personal experience all the nuances of using products with retinol, and which of them really work. In the photo above are the best products with retinol (one of the many that I have tried), which are produced by SkinCeuticals (USA) and ZO® Skin Health (USA). And these companies truly produce the most effective products with pure retinol - compared to many other products I have tried.
In this article we will talk about the criteria for choosing retinol products for the face so that they are truly effective. And of course, the main criteria will be the choice of the correct form of retinol, as well as its correct concentration. We will also talk about the duration of courses for correcting age-related changes using cosmetics with retinol, and when you can notice the first visible results.
Nosological classification (ICD-10)
- A09 Diarrhea and gastroenteritis of presumably infectious origin (dysentery, bacterial diarrhea)
- A15-A19 Tuberculosis
- B05 Measles
- E50 Vitamin A deficiency
- E50.0 Vitamin A deficiency with conjunctival xerosis
- E50.4 Vitamin A deficiency with keratomalacia
- E50.5 Vitamin A deficiency with night blindness
- E55.0 Active rickets
- H01.1 Non-infectious dermatoses of the eyelid
- H10.1 Acute atopic conjunctivitis
- H10.9 Conjunctivitis, unspecified
- H16 Keratitis
- J04 Acute laryngitis and tracheitis
- J06 Acute upper respiratory tract infections of multiple and unspecified localization
- J18 Pneumonia without specifying the pathogen
- J20 Acute bronchitis
- J22 Acute respiratory infection of the lower respiratory tract, unspecified
- J39.9 Upper respiratory tract disease, unspecified
- J42 Chronic bronchitis, unspecified
- J44.9 Chronic obstructive pulmonary disease, unspecified
- K20 Esophagitis
- K25 Stomach ulcer
- K26 Duodenal ulcer
- K29.5 Chronic gastritis, unspecified
- K29.9 Gastroduodenitis, unspecified
- K52 Other non-infectious gastroenteritis and colitis
- K74 Fibrosis and cirrhosis of the liver
- L11.0 Acquired keratosis follicularis
- L30.9 Dermatitis, unspecified
- L40 Psoriasis
- L44.0 Pityriasis red hairy pityriasis
- Q80 Congenital ichthyosis
- T14.1 Open wound of unspecified body area
- T30 Thermal and chemical burns of unspecified location
- T33-T35 Frostbite
What retinoids to use for acne
Having understood how retinol works for acne, the question arises: what form of retinol is best to use to treat acne?
To answer this question, you need to understand:
- When treating acne, the goal is not to activate fibroblasts and basal keratinocytes to stimulate cellular renewal and synthesis of the dermal matrix.
- With acne, skin barriers are often compromised. Therefore, the requirement for the selected Retinoid is to minimize aggression and eliminate irritating effects that could provoke the client’s desire to refuse therapy.
Irritation from retinol
Conclusion
At the beginning of therapy, give preference to atraumatic forms of Retinoids without affecting RAR receptors (fibroblasts and basal keratinocytes). Pure retinol and retinol acetate are excluded from acne therapy, especially in the initial stages of treatment.
Composition and release form
| Oral solution | 1 ml |
| retinol palmitate | 100000 IU |
| (1 drop of solution from a dropper or eye dropper contains 3300 IU) | |
| 1 mg of retinol palmitate corresponds to 1817 IU | |
| excipients: butylated hydroxytoluene; butylated hydroxyanisole; rapeseed oil |
in dark glass bottles of 10 ml; in a cardboard pack 1 bottle or in dark glass bottles of 10 ml, complete with a dropper; 1 set in a cardboard pack.
What are retinol and retinoids
Retinoids are a group of substances derived from Vitamin A. They are one of the most researched ingredients and have long been used in dermatological practice with many medical studies around the world and evidence base for their effectiveness!
Retinol is one of the forms of retinoids, however, in everyday life, all representatives of the retinoid group are called “retinol”.
This is not true!
Retinoids include:
- Retinol in its pure form,
- Retinol esters (retinol acetate and palmitate),
- Retinoic acid,
- Retinaldehyde.
Indications for the drug Retinol palmitate
Vitamin A deficiency (hypo- and avitaminosis A); eye diseases (retinitis pigmentosa, xerophthalmia, hemeralopia, keratomalacia, conjunctivitis, eczematous lesions of the eyelids), skin diseases accompanied by dryness and delayed epithelization (ichthyosis, ichthyosiform erythroderma, psoriasis, variable erythrokeratoderma, keratoderma, lichen planus pilaris (Devergie's disease), acne, seborrhea, hair diseases, neurodermatitis, follicular keratosis, superciliary ulerythema, baldness, burns, wounds, frostbite, epidermolysis bullosa, congenital pachyonychia, leukoplakia, familial benign pemphigus Hailey-Hailey, Darier's follicular dyskeratosis), skin tuberculosis; infectious and colds (measles, pneumonia, dysentery, tracheitis, bronchitis, acute respiratory infections), rickets, malnutrition, erosive gastroduodenitis, gastric and duodenal ulcers, cirrhosis of the liver (as part of complex therapy).
Products with retinol: price
The world's leading manufacturers of cosmetics with pure retinol are definitely SKINCEUTICALS® and ZO® SKIN HEALTH. But we immediately warn you that the products of these companies are not cheap - from 6,500 rubles and above. In Kiehl's branded cosmetics stores, you can find a good cream-serum with retinol, Kiehl's Retinol Skin-Renewing Daily Micro-Dose Serum (Serum with a microdose of retinol for every day to combat the signs of skin aging). The cost of this serum is from 4300 rubles per 30 ml. More details about all these tools can be found in the link below.
Good cosmetics with retinol -
Products that contain 0.1% pure retinol + 0.1-0.2% retinol esters are available for purchase at the pharmacy (their cost will be from 2400 to 2700 rubles). In addition, on sites such as Amazon or Ebay, you can purchase products with pure retinol or retinaldehyde from another leading manufacturer, SIRCUIT® (a cream or serum from this company will cost $80).
And on the iHerb website you can purchase American and Neutrogena cosmetics for about 2,000 rubles. These are also well-known manufacturers of cosmetics with retinol, but they do not indicate the percentage of pure retinol in their products. At the link below, you can read the rating of the best products with retinol (according to our editors), as well as familiarize yourself with the composition and characteristics of these products.
→ The best products with retinol for facial skin
Side effects
Rarely - manifestations of hypervitaminosis A: in adults - drowsiness, lethargy, headache, facial flushing followed by peeling, nausea, vomiting, possible exacerbation of liver disease, gait disturbance, pain in the bones of the lower extremities; in children - short-term increase in body temperature, drowsiness, increased sweating, vomiting, skin rashes. Increased intracranial pressure (infants may develop hydrocephalus, protrusion of the fontanel).
With a dose reduction or temporary discontinuation of the drug, side effects disappear on their own. In some cases, on the first day of use, itchy maculopapular rashes may occur, requiring discontinuation of the drug.
When high doses are prescribed for skin diseases, after 7–10 days of treatment, an exacerbation of the local inflammatory reaction is observed, which does not require additional treatment and subsequently decreases. This effect is associated with the myelo- and immunostimulating effects of the drug.
Skin aging is a continuous process that affects the appearance and function of the skin. The course of this process is determined by internal factors (genetic) and external (state of the environment and lifestyle) [1, 2]. Exposure of skin cells to reactive oxygen species, cellular stress, slowdown of metabolism in cells and tissues reduces skin regeneration and repair. Typical signs of skin aging are dryness and flaking, hyperkeratosis, decreased immune and protective functions of the skin and, as a consequence, the appearance of age-related pigmentation and neoplasms [3, 4]. Scientific research in recent years shows that topical retinoids are strategically important antiage
-therapy, prevention of photoaging and treatment of photodamage [5, 6].
Retinoids are structural analogs of vitamin A. Retinoids have been successfully used in clinical practice for more than 60 years. During this time, three generations of retinoids appeared, and the number of drugs containing them exceeded 2500. Today in dermatology there are more than 125 pathological conditions for which the prescription of retinoids can be effective.
Retinol is one of the most famous representatives of the 1st generation of retinoids. Preparations based on it are in the arsenal of every Russian dermatologist. Although multicenter studies have not been conducted to evaluate the effectiveness of retinol, there are many studies that evaluate the biological and clinical effectiveness of this substance [7, 8].
Commonly known as vitamin A, retinol belongs to the family of endogenous natural retinoids and is a precursor to retinaldehyde and trans-retinoic acid. Despite the fact that retinol is a precursor of retinoic acid, in foreign practice since 1984 it has been predominantly used in the production of cosmetic products and over-the-counter products [9].
However, it should be borne in mind that in proper dosages, retinol has pronounced biological activity and has a significant clinical effect, especially in the correction of pathological conditions directly or indirectly associated with exposure to ultraviolet radiation. A study (R. Kafi et al., 2007) [10] demonstrated that the use of retinol in older people significantly improved the appearance of the skin of areas of the body not protected from exposure to sunlight. A. Rawlings et al. [11] in a randomized study conducted over 12 weeks, confirmed the effectiveness of retinol palmitate for the prevention of chrono- and photoaging compared to the control group ( p
<0,001).
Considering the minimal side effects of retinol, its use may become one of the priority options for solving such a problem as the tactics of managing “aged” patients with various skin pathologies. Older people are characterized by dry and flaky skin: as they age, skin dryness increases and oiliness decreases. These changes may be partly due to age-related impairments in barrier function: a decrease in lipid content, as well as filaggrin in the epithelium, which ultimately increases transepidermal fluid loss (TEFL) [12]. Almost all forms of hand eczema in older people begin with a violation of the stratum corneum barrier, which is accompanied by TPE [13]. In “aged” patients, thinning of the epidermis is realized mainly due to a decrease in the thickness of the spinous layer and partial or complete disappearance of the granular layer. In old age, the stratum spinosum may consist of two rows of cells. In the epidermis, the number of Langerhans cells decreases; in those that remain, dystrophic changes are noted (clearing of the matrix, cytoplasm), and sometimes partial cell lysis, which leads to a sharp decrease in the protective properties of the epidermis.
Retinoids are well known for their ability to influence a number of cellular processes, such as cell growth and differentiation, apoptosis and embryonic development, and immunomodulation. Many of the effects, including retinol, are explained by the result of their interaction with specific receptors for retinoic acid and the existence of retinoid-binding proteins (Fig. 1)
[14].
Figure 1. Interaction of retinol with specific retinoic acid receptors and retinoid-binding proteins.
Thus, when using retinol with antioxidants (vitamins C, E, zinc), an improvement in the barrier function of the skin and an increase in the activity of immune system cells were noted [15, 16]. In their study, J. Fluhr et al. [17] confirmed that the use of retinol for 2 weeks significantly reduces transepidermal water loss, which directly indicates an improvement in the barrier properties of the skin. Experimental results [18] have proven that the use of 1.6% retinol on normal human skin causes thickening of the epidermis and increases the expression of CRABP II and CRBP (retinoid-binding proteins) mRNA. Today it is known that UVR activates the expression of matrix metalloproteinase (MMP) genes. As a result, the formation of collagenase, gelatinase and stromelysin, MMP enzymes that destroy collagen, is activated [19-21]. The decrease in type I collagen content under the influence of UV irradiation is also explained by the activation of MMPs. More recently, it has been demonstrated that, in addition to the numerous mechanisms of action of retinoids, the anti-inflammatory effect of vitamin A derivatives is realized by suppressing the toll-like receptor system (TLR-2). Given the proinflammatory nature of UV-induced aging, it is possible that TLR-2 also mediates skin changes during aging. Since TLR-2 regulates MMP expression, it can be assumed that the effect of topical retinoids is partly realized through suppression of MMP expression due to inhibition of the TLR-2 system [22]. J. Varani et al. [23] studied the effects of topical application of 1% retinol in individuals aged 80 years and older ( n
=53) with characteristic age-related skin changes. The authors [23, 36] noted that the use of retinol for 7 days inhibited the activity of MMP, collagenase and gelatinase with a corresponding increase in collagen synthesis by fibroblasts in the tissue samples studied. S. Seité et al. [16] conducted two double-blind, placebo-controlled clinical trials in postmenopausal women. The results of external use of 0.04 and 0.07% retinol in combination with 3 and 3.5% vitamin C were assessed after 3 and 6 months. After 3 months, the main changes were recorded in the epidermis (the severity of hyperkeratosis decreased and the number of rows of the Malpighian layer increased). After 6 months, positive structural changes were noted in the dermoepidermal junction, the content of type I collagen increased, which led to a change in the ratio of collagen types I and III.
To date, it has been proven that retinol interacts with nuclear receptor systems (RARs) and during metabolism can be converted into tretinoin, which is a hormone [18]. Nuclear receptors RARs and RXRs belong to a large superfamily of nuclear hormone-sensitive receptors, which include receptors for steroids, thyroid hormones and vitamin D. Obviously, the interaction of these receptors is being actively studied in connection with the use of topical and systemic retinoids for the treatment of allergic dermatoses resistant to traditional treatment with topical glucocorticosteroids and UV therapy [24-26].
In our country, one of the external products that contain retinol is Redecil ointment. Redecil
- a new combined dermatotropic drug, which contains 0.5% retinol palmitate and 3% dioxomethyl-tetrahydropyrimidine (methyluracil) on an emulsion basis, was specially developed for the treatment of allergic skin diseases.
Indications for the use of Redecil
include eczema, neurodermatitis, and atopic dermatitis.
IN AND. Albanova et al. [27, 28] assessed the effectiveness of Redecil
in the treatment of atopic dermatitis and noted its anti-inflammatory and anti-allergenic properties, as well as its effect on the main skin symptoms.
Redecil
ointment reduced dryness by 30%, reduced swelling by 35%, skin lichenification by 50%, itching by 50%, and the incidence of concomitant skin infection by 50%, while other parameters remained at the same level.
Research results [29] showed that Redecil
stimulates the proliferation of epidermal cells and modifies the inflammatory process, activating the fibroblastic reaction of the dermis;
At the same time, the combination of intensive skin regeneration with the absence of manifestations of hyperkeratosis, noted during the study of the proposed dosage form, seems important. One of the notable molecular mechanisms of action of retinol is the increase in keratinocyte proliferation activity by triggering epidermal growth factor. This factor is involved in the healing of skin wounds, which is extremely important for elderly patients receiving chemotherapy [30]. Since Redecil
contains methyluracil (a structural analogue of the natural nucleotide - thymine), which is a known stimulator of regeneration and has anabolic, immunomodulatory and anti-inflammatory effects, the range of use of the ointment is significantly expanded
(Fig. 2)
[29, 31].
Figure 2. Effects of using Redecil ointment. Thus, the use of Redecil
in surgical practice has made it possible to optimize the timing of treatment, especially for burns and the treatment of purulent and infected wounds, to achieve earlier regeneration in trophic ulcers and faster healing [32].
It is believed that the effectiveness of retinol is 20 times weaker than tretinoin. However, it has been proven that retinol, used without an occlusive dressing, penetrates the skin more intensively than retinoic acid under the same conditions [12]. Thus, retinol at a concentration of 0.25% can be an effective treatment when applied to the skin. At this concentration, retinol does not irritate the skin, but at the same time induces cellular and molecular changes similar to those observed when 0.025% retinoic acid is applied to the skin. When retinol is applied at this concentration, histological and molecular changes are observed in the skin, similar to those when retinoic acid is applied [8]. Another important circumstance: when applying retinol ( Redecila
) the total level of retinoic acid in the body does not increase significantly [33].
In addition, Redecil
does not cause statistically significant changes in hemoglobin content, cellular composition of peripheral blood and other biochemical parameters reflecting the state of protein, lipid, carbohydrate and mineral metabolism [33]. This observation suggests that when applied topically, the absorption of retinol palmitate is minimal, due to which there is a fairly wide range of therapeutic effects and age range. Although retinol interacts with RARs and can be metabolized into tretinoin, erythema has rarely been reported with retinol [12, 34, 35].
Thus, based on literature data, we can conclude that retinol is an effective and relatively safe agent in the treatment of aging and photoaging of the skin. New drug for external use Redecil
has anti-inflammatory, antipruritic, softening and immunomodulatory effects, affects the reparative function of the skin.
Redecil
is easy to use, suitable for long-term use without reducing therapeutic activity and has virtually no side effects.
Directions for use and doses
Inside, after eating early in the morning or late in the evening.
For mild to moderate vitamin deficiency: adults - up to 33,000 IU/day; children - 1000–5000 IU/day depending on age.
For eye diseases (hemeralopia, xerophthalmia, retinitis pigmentosa): adults - 50,000–100,000 IU/day and at the same time 0.02 g of riboflavin.
For skin diseases: adults - 50,000–100,000 IU/day; for acne and ichthyosiform erythroderma - 100,000–300,000 IU/day. Children are prescribed at a rate of 5000–10000 IU/kg per day.
In gastroenterology - 50,000 IU per day.
Single doses of retinol palmitate for adults should not exceed 50,000 IU and for children - 5,000 IU. Daily doses for adults are 100,000 IU and for children - 20,000 IU.
How does retinol work for acne?
Points of application of retinol and its derivatives for acne:
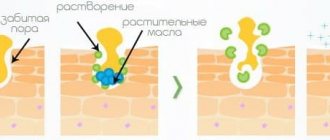
FOLLICULAR HYPERKERATOSIS
Retinoids, like AHA acids, are able to break the bonds between keratinocytes, stimulating their exfoliation, inhibit the excessive proliferation of the ductal epithelium, thereby cleanse the pores on the face and eliminate their blockage.
CLOSED COMEDONS
Through the hair follicle, retinoids are able to penetrate right up to the ducts of the sebaceous glands, where they also stimulate exfoliation and elimination of accumulated sebum, which stretches the sebaceous glands, turning them into retention cysts.
Result : a large number of dead cells do not accumulate in the ducts and their removal to the outside improves, which removes the blockage of the duct - sebum accumulated in the gland comes to the surface of the skin.
INFLAMMATION
Retinoids are antioxidants that further reduce the production of proinflammatory cytokines and other inflammatory factors (eg, IL-1β, TNF-α, and nitric oxide NO).
Important : inflammation is recognized as a key factor provoking the severity of the acne process, and, therefore, the main starting point for acne therapy.
PATIENT
Retinoids indirectly inhibit the proliferation of P. acne bacteria, preventing the formation of antibiotic resistance in bacteria that form skin microbiologists.
IMMUNE FUNCTION OF THE SKIN
Retinoids block important inflammatory pathways such as AP-1, as well as leukocyte migration and toll-like receptors. In addition, retinoic acid (one of the forms of retinol, formed inside the skin during the transformation of retinol) affects Langerhans cells - skin macrophages, increasing their readiness for phagocytosis and migration to the site of inflammation.
PREVENTION OF POST-ACNE
According to clinical observations, early use of retinoids to correct acne minimizes the risk of scarring.
Also, topical retinoids reduce the risk and clinical manifestation of post-acne hyperpigmentation. The higher the dose of topical retinoids, the greater the preventive effect.