As is known, mites of the genus Demodex are often considered the etiological and pathogenetic agent in the development of papulopustular dermatoses. An important point is that mites, complicating existing skin diseases, reduce the clinical effect of therapy, thus contributing to the transition of dermatoses to a chronic form. An additional difficulty for antiparasitic therapy is created by the structural features of mites, which makes it necessary to prescribe long courses of therapy and select drugs with a minimum molecular size. The effect of the drug is hampered by the dense cuticle covering the body of the mites, which has three layers: the outer layer is the epicuticle, the middle layer is the exocuticle and the inner layer is the endocuticle. The exo- and endocuticle are impenetrable, so the body of the mite is difficult to access by large molecules of exogenous substances, incl. for acaricidal drugs. Communication with the external environment of ticks occurs through water or gas exchange [3].
In order to achieve the elimination of ticks, antiparasitic (acaricidal) drugs are used. Over the years, metronidazole, which is a derivative of the nitroimidazole group, has proven the greatest clinical effectiveness. This drug is prescribed for a course of 4 to 6 weeks [7, 29]. It has been established that metronidazole enhances the protective and regenerative functions of the mucous membrane of the stomach and intestines [2, 4] and causes a pronounced anti-edematous effect [30]. The drug has a bacteriostatic effect, complicating the DNA synthesis processes of gram-negative anaerobic bacteria [13, 38], and is also antiparasitic against Demodex folliculorum [2].
Studies by DI Grove (1997) and PG Nielsen (1988) have proven the suppressive effect of the drug on some indicators of cellular immunity, in particular the suppression of leukocyte chemotaxis [26, 32]. The drug has an immunomodulatory effect due to the inhibition of vascular endothelial growth factors, preventing neoangiogenesis [15]. Tolerability of the drug is generally satisfactory. Side effects include headache, nausea, vomiting, dry mouth, urticaria, itching, leukopenia, candidiasis [13].
A.A. Frankenberg (2007) notes that in recent years, failures in the treatment of demodicosis with metronidazole have increased significantly. In his opinion, the ineffectiveness of therapy may be associated with the development of resistance of bacterial-parasitic flora to metronidazole, which has been used for more than 40 years [16]. As an alternative method of treating demodicosis, Ya.A. Yutskovskaya (2010) suggested using metronidazole topically. The study showed significant clinical improvement, which was manifested in a decrease in erythema, the number of papulopustular elements and the severity of the inflammatory process. According to the authors, laboratory elimination of mites after 14–21 days reached 2–3 mites in a scraping per 1 cm2 [17].
From the group of other synthetic antibacterial agents, the 5-nitroimidazole derivative ornidazole is widely used in cycles of 8 to 10 days. The drug has both antiparasitic and bacteriostatic effects, increases the activity of neutrophils, stimulates adrenergic structures, and enhances reparative processes [4, 18].
When comparing the effectiveness of the drugs ornidazole and metronidazole A.A. Frankenberg et al. (2007) the following results were obtained: the therapeutic effect when using ornidazole occurs almost 2 times faster compared to metronidazole; patient tolerability of the drug is satisfactory; minor side effects were noted, among which the most common were nausea and a metallic taste in the mouth; The blood and urine test results of the patients before and after treatment were within normal limits. When treated with metronidazole, side effects were observed more often, including: nausea, metallic taste in the mouth, dizziness, and the development of candidiasis. During 9 months of observation of patients taking ornidazole, there was no relapse [9, 16].
When choosing local treatment for demodicosis, one should take into account the general principles of external therapy used in dermatology. In some cases, etiotropic therapy should be immediately prescribed; in some cases, symptomatic therapy should be started, aimed at eliminating and resolving acute inflammatory manifestations and accompanying subjective sensations. Strict personalization of external treatment and constant monitoring of the patient's condition are necessary. In acute and subacute forms of the inflammatory process, you should first use dosage forms with a surface action of agents (lotions, shaken suspensions, pastes). After eliminating the acute inflammatory phenomena, the next stage is to switch to the ointment form of the drug, which acts directly on the etiological factor.
In external therapy, drugs containing metronidazole 1% in the form of an ointment or gel are most often used for 14 days. Metronidazole acts on the body's nonspecific resistance and affects cell-mediated immunity [33, 35]. As an alternative therapy, topical application of 10% benzyl benzoate ointment at night is possible [1, 6, 23]. Demoten gel (sulfur, hyaluronic acid, AloeVera juice, polyvinylpyrrolidone) for the treatment of patients with demodicosis and rosacea was highly praised [14].
In special cases, pathogenetic treatment is carried out for demodicosis. For example, in the case of acneiform type demodicosis or resistance to antiparasitic drugs, it is advisable to use systemic retinoids (isotretinoin) at a dosage of 0.1–0.5 mg/kg body weight per day for 2–4 months [24].
For the treatment of demodecosis of the periorbital region, alcohol-ether mixtures, 3–5% trichopolum cream, sodium sulfapyrazine, anticholinesterase agents (cholinomimetics): physostigmine, 0.02% phosphakol, 0.01% armin, 0.5% - ny tosmilen [11]. Good treatment results are observed with the use of blepharogel-1 and -2, blepharolotion [12].
Recently, dermatological practice has been significantly enriched with new drugs, significantly increasing the possibilities of choice in the treatment of patients with parasitic dermatoses. The drug Spregal, containing a solution of esdepaletrin and piperonyl butoxide, showed high effectiveness. It is used on the affected areas of the skin, rubbing with a swab 1-3 times a day. The drug is well tolerated and does not cause serious side effects [5, 8].
Permethrin (a group of pyrethroids) also has antiparasitic properties. Pyrethroids bind to the lipid structures of nerve cell membranes, disrupting the functioning of sodium channels that regulate membrane polarization. Repolarization of the membrane is hindered, which paralyzes the parasite. The important point is when pyrethroid molecules are able to penetrate the tick cuticle and concentrate in the hemolymph [3]. Permethrin 5% cream is applied twice daily for 15–30 days [31, 37]. However, we must remember that the permeability of different areas of the skin is not the same. Medicinal substances penetrate most actively into the skin of the face, where the thickness of the stratum corneum is minimal, so the rapid development of side effects in the form of erythema and simple contact dermatitis is possible.
The drugs ivermectin, lindane 1%, and crotamiton 10% also have acaricidal activity [23, 29]. Ivermectin is a synthetic derivative of compounds with antiparasitic activity known as avermectins. The drug is effective against endoparasites with tropism for the skin (Strongyloides stercoralis, Ancylostoma braziliense, Cochliomyia hominivorax, Dermatobia hominis, Filaria bancrofti, Wucheria malayi, Onchocerca volvulus, Loa-loa) and ectoparasites (Sarcoptes scabies, Pediculus humanus, Demodex folliculorum and Cheyletiella spr.) [22]. Foreign studies recommend using ivermectin systemically or topically in the form of a 1% cream. Studies have proven that ivermectin has antiparasitic and anti-inflammatory effects. Clinical improvement with topical 1% ivermectin cream was observed after 12 weeks of therapy [27]. The drug is administered orally at a dose of 200 mg/kg body weight twice with a break of 7 days [28]. However, in Russia this drug is used only for the treatment of demodicosis in animals. The use of 1% lindane also raises many doubts due to its neurotoxicity, therefore the drug is banned in a number of countries, and in some its use is limited [21]. As for the drug crotamiton 10%, it is applied to the skin at night for two to three days and is quite often used in pediatric practice [20, 34].
Among physiotherapeutic techniques, it is recommended to use the properties of narrow-band blue light (405–420 nm). The wavelengths of blue light are slightly longer than those of ultraviolet radiation, so narrow-band blue light reaches the reticular layer of the dermis, penetrating to a depth of 2.5 mm, corresponding to the location of the sebaceous glands. Single observations indicate the high effectiveness of this method in the treatment of acne complicated by demodicosis [10]. Some studies have proven the positive effect of using intense pulsed light (IPL - Intensive Pulse Light), discovered in 1992 and having a wavelength from 515 to 1200 nm [25]. IPL radiation suppresses the secretion of the sebaceous glands with their subsequent involution, which leads to the resorption of lymphocytic infiltrates and the death of mites [36].
Cryotherapy has an antidemodic effect, and to achieve a more lasting therapeutic effect, it is recommended to use cryotherapy in combination with external preparations containing metronidazole [1, 19].
Despite the fact that, according to various authors, the current “gold” standard and most effective method of treating demodicosis is the systemic use of the antiparasitic drug metronidazole, the drug itself has many side effects and has a number of contraindications. Since the search for new therapeutic agents that have the least negative effect on the body remains a pressing topic in medicine, we assessed the effectiveness of external therapy for demodicosis in comparison with the systemic use of drugs.
The purpose of this study: to compare the traditional treatment regimen for demodicosis of the facial skin (250 mg metronidazole orally 2 times a day; topically - 1% metronidazole cream once a day for 20 days) with the effectiveness of topical therapy (7% metronidazole cream topically for 20 days).
Material and methods
The study included 64 patients with acne and rosacea complicated by demodicosis. The diagnosis of acne and rosacea was made at the initial appointment based on the clinical picture of the diseases. At the same time, the main complaints of patients were taken into account, divided into the following groups: rashes, pain, burning, redness, itching, pigmentation, the presence of crusts/excoriations, telangiectasia, oily sheen. When assessing the local status (status localis), the following primary and secondary morphological elements were identified: papules, pustules, open comedones, milia, telangiectasia, crusts, redness, pigmentation, oily sheen. Each morphological element was counted and the clinical picture as a whole was assessed for the presence of perifocal erythema and oily sheen of the facial skin in patients before and after treatment. All patients included in the study were examined for the presence of Demodex mites by scraping the facial skin and squeezing out the contents of the sebaceous glands before and after treatment. The diagnosis of demodicosis was established when more than 5 mites per 1 cm2 were detected. The study included men and women over 18 years of age with no somatic complications and upon signing informed consent to participate in the study.
All patients were divided into two equal groups depending on the chosen treatment method. Patients of the first group (n=32) received 250 mg of metronidazole orally 2 times a day, externally - 1% metronidazole once a day for 20 days, patients of the second group (n=32) received 7% metronidazole externally in within 20 days. The treatment method was chosen randomly.
Statistical data processing was performed using the SPSS-21 software package. The relationship between categorical indicators was determined by Fisher's exact method. Fisher's exact test is a test of statistical significance used in the analysis of categorical data when sample sizes are small. To assess the significance of differences in follicle sizes, one-way analysis of variance with pairwise comparisons was used.
Research results
Of all the patients included in the study, 38 (59.37%) had acne and 26 (40.62%) had rosacea. The distribution by gender, age and diagnosis is presented in Table. 1.
The patients' return visit took place after 20 days of continuous therapy. Subjectively, both treatment regimens were well tolerated by the patients, no side effects were noted, and none of the patients were excluded from the observation group. Evaluation of the effectiveness of therapy was based on patient complaints and clinical picture. As can be seen from table. 2, after treatment there was a statistically significant decrease in patient complaints of rashes, burning, pain, itching, and redness. Moreover, in patients of the second group, complaints about oily skin decreased, which is an additional advantage of topical therapy.
Analysis of clinical manifestations after therapy showed that the number of the following morphological elements in patients of the first and second groups significantly decreased: papules, pustules, perifocal erythema, excoriations (p = 0.005) compared to the initial data (Fig. 1, 2).
When repeated scraping for the presence of Demodeх mites in two groups, the following data were obtained: in the first group, mites were found in 19 (30%) patients, in the second - in 20 (32%), i.e. mites of the genus Demodex after treatment in the two groups were found in approximately equal numbers of cases.
Thus, assessing the results of treatment, we can state that the effectiveness of therapy in both groups was the same. Analysis of the clinical picture showed a positive dynamics of therapy, which was manifested in a significant decrease in the number of morphological elements characterizing the severity of inflammation. The effectiveness of therapy was confirmed by a decrease in subjective complaints of patients after treatment, and in patients who received only external therapy, complaints about oily skin decreased, which is an additional advantage. Thus, clinical observations have demonstrated the lack of superiority in systemic therapy of demodicosis compared to external therapy using a drug containing 7% metronidazole in the form of a cream or cream-gel, which was confirmed by the results of statistical analysis.
conclusions
Our study showed that the use of a topical product containing 7% metronidazole for 20 days by patients with demodicosis is comparable in effectiveness to systemic treatment with metronidazole 250 mg orally for 20 days. External use of 7% metronidazole makes it possible to avoid polypharmacy and systemic administration of the drug, which reduces the risk of developing side effects of therapy.
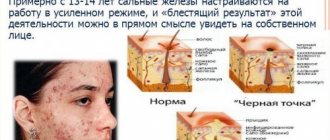
Symptoms
Since there is demodicosis of the eyelids (eye form) and a skin disease, there will be different types of symptoms for these two forms.
Symptoms of demodicosis on the skin are manifested by the following:
- acne: from nodules and pustules to rosacea;
- a feeling of itching that causes severe discomfort. It manifests itself most strongly at night and in the evening;
- increased skin oiliness. It is the greasy environment that best promotes the proliferation of ticks;
- red areas of the skin, which indicate increased pressure in the blood vessels. It is associated with inflammation of the skin;
- growth of the wings of the nose. In advanced cases, they increase in size as the functioning tissue is replaced by connective tissue.
The following symptoms are typical for the ocular form of the disease:
- eye fatigue. It is caused by inflammation and the fact that the patient is forced to constantly focus his vision and strain;
- eyelash loss. This is explained by the fact that the mite attacks the hair follicles;
- sticking of eyelashes. The formation of a thin film along the eyelash growth line due to inflammation is precisely the reason for this undesirable effect;
- redness and inflammation of the eyelids. In many cases, this greatly complicates the patient’s life and reduces the level of comfort.
Since some of these signs may indicate other diseases, demodicosis in humans requires additional research methods to make an accurate diagnosis.
Do you have symptoms of demodicosis?
Only a doctor can accurately diagnose the disease. Don't delay your consultation - call
Diagnostics
To determine the disease, the patient requires a visual examination. The doctor then interviews the patient and orders a laboratory test. The materials that are taken for research (scrapings) are examined using microscopy - but the diagnosis of demodicosis does not end there. It happens that the result is negative - after which it is prescribed again. This is due to the fact that ticks are especially active in the evening and at night, and the analysis itself is usually taken in the morning, which can reduce the accuracy of the results. In addition, they may be affected by certain cosmetics - the skin should not be treated before the test.
The material is collected not only by scraping. To study the eye shape, several eyelashes are taken from the patient, and there is also a study using a special adhesive tape, which is stuck on at night and checked in the morning.
The examination of the material under a microscope itself takes only a few minutes, so the patient receives the result almost immediately.
Question answer
Is demodicosis contagious?
Yes, you can become infected with demodicosis through kissing, hugging, using the infected person’s things, his hygiene products, etc. But this does not mean that you will show signs of illness. As we have already said, the tick is found in almost all adults, it’s just that most are carriers. For the development of the disease, other additional factors are needed.
Is it possible to get demodicosis from animals?
Animals, like people, suffer from this mite. However, there are several dozen types of pathogens - and each lives only on its own host. In other conditions it dies. Therefore, you cannot catch the disease from a dog or other animal.
Which pillows are best for preventing demodicosis?
It is best to choose synthetic fabrics to prevent demodicosis. The mite lives well in feather and down pillows, but it is extremely difficult for it to take root in synthetic ones, especially those that are regularly cleaned.