Pityriasis versicolor is a fungal infection of the skin with certain symptoms that occurs as a result of the malassezia fungus entering the body. It is often diagnosed in countries and regions with warm to hot climates, which is why it is called beach lichen.
This skin disease appears in adolescents and young adults (it is extremely rarely diagnosed in preschool and retirement age), but people prone to dermatomycosis are also at risk. The disease is long-term and protracted; relapses occur (especially in the hot season, regardless of the region of residence), so it is often called chronic.
Ringworm, like many fungal and viral diseases, is rarely a serious threat to life, but it can indicate health problems and reduce quality of life, especially affecting a person's psychological state.
Causes of tinea versicolor
The content of the article
Ringworm affects middle-aged people. Medicine identifies the causes that lead to the appearance of this disease in humans. These include:
- Predisposition to fungal skin diseases.
- Disruptions in the course of physiological processes in the epidermis.
- Endocrine diseases.
- Lack of a good night's sleep.
- Lack of rest.
- Time zone change.
- Excessive hygiene, using antiseptics.
- Improper functioning of the human immune system.
- Frequent bathing in salt water.
- Lack or excess of vitamins.
- Wearing clothes made of synthetic materials.
- Improper functioning of the lymphatic drainage system.
- Long-term use of steroid hormones.
- Nervous system problems.
- Hormone imbalance.
- Lack of hygiene measures in public places.
Tinea versicolor: possibilities of using shampoo containing ketoconazole and zinc pyrithione
Pityriasis versicolor (pityriasis versicolor) is a common superficial skin lesion caused by lipophilic fungi of the genus Malassezia [1]. Fungi of this genus are the only representatives of the fungal kingdom that are commensals of normal human skin [2]. It is believed that at least 90% of the entire population of the Earth are carriers of Malassezia, and approximately up to 10% of the planet's inhabitants are affected by it, although the disease is considered opportunistic and not contagious. The intensity of colonization changes with age: it is extremely low in newborns and then gradually increases towards puberty, as the activity of the sebaceous glands increases [3]. In the population, the incidence statistically depends on: – age (peak incidence is at the age of 14–40 years) [2]; – gender differences (men get sick 1.5–2 times more often) [2]; – the presence of concomitant diseases of the gastrointestinal tract, endocrine disorders, vegetative diseases, immunodeficiencies of various etiologies [2]; – geographic latitude (in temperate climates – about 2%, in tropical climates – up to 40% of the total population) [4]; – professional activity of patients (in persons engaged in physical labor and sweating heavily) [3]; – hereditary predisposition [1]. The above factors significantly influence the composition of the sweat-fat mantle. A change in the chemical composition of sebum, favorable for the fungus, is an increase in the concentration of oleic, palmitic, linoleic, linolenic, stearic, and myristic fatty acids [2]. The favorite place of localization is the skin of the chest and back; less often, elements are noted on the skin of the neck, abdomen, lateral surfaces of the torso, and the outer surface of the shoulders. In addition, rashes can be found on the scalp, but without affecting the hair, sometimes in the groin folds and axillary areas. The disease is manifested by the appearance of pinkish-brown spots with slight pityriasis-like peeling without inflammation and subjective sensations (rarely - slight itching). Merging, the spots can form quite large lesions with scalloped borders. Their color gradually becomes darkish brown. The spots do not protrude above the skin level, and their surface is covered with small pityriasis-like scales. Insolation and ultraviolet irradiation have a detrimental effect on the colonies of the pathogen, and the skin under them does not tan, and white spots (pseudo-leukoderma) appear against the background of a general tan [5]. In addition to the classic course, there are also atypical forms of lichen versicolor: erythematous-squamous, lichenoid, urticaria-like, erythrasma type, vitiligo, diffuse, circinate, as well as special forms: Malassezia folliculitis and the so-called black form [2]. A study of the clinical forms of lichen versicolor shows that the most common (≈90%) is the classical form of the disease, less often - atypical clinical variants of lichen versicolor. The widespread form of the lesion (≈80%) and typical localization of the rash (≈90%) predominate. Knowledge of atypical clinical variants and localizations of pityriasis versicolor is necessary for timely diagnosis and effective treatment of the disease [6]. Verification of the diagnosis is carried out: • anamnestiically; • according to the clinical picture; • detection of hidden peeling of the skin (Balzer test with 5% iodine solution); • microscopy of scales from lesions; • using examination under the rays of a Wood's lamp [1, 7]. Tinea versicolor is usually well treated with topical antimycotics. The US FDA has not approved any systemic drugs for its treatment for a long time, even though some of these drugs have already been included in clinical guidelines [8]. Among the traditionally used treatment methods, such as Demyanovich treatment are not currently used, and antiseptics such as 2% alcohol solution of iodine or 2% salicylic alcohol are used along with modern antimycotics. Along with antifungal creams, ketoconazole in the form of 2% shampoo should be noted. The use of external forms that allow covering a significant surface of the body is of no small importance in the treatment of lichen versicolor. Even with individual small lesions, it is recommended to treat all areas where lichen versicolor usually develops. The shampoo is used once a day for 5 days [9]. Ketoconazole in the form of shampoo as a drug for the treatment of lichen versicolor was included in the clinical recommendations of the 2010 RODVC [10] and is widely used in world practice [11].
But there are also some features of the mycosis under study, which increasingly force one to turn to systemic and combination therapy. First of all, these are recurrent, widespread and atypical forms of the disease, as well as cases of failure of local therapy. The most important problem of local therapy is the impossibility of 100% visual control of the treatment of lesions, since the pathogen can remain in subclinical quantities in places that patients do not treat during treatment for various reasons. This is especially true for men, who are initially generally recognized to be less compliant with external therapy, although they get sick more often. Therefore, the level of relapses of lichen versicolor is at least 20% after local treatment, and, according to some data, the number of patients with relapses of this pathology after treatment varies from 60% in the first year of observation to 90% over 2 years, more often with immunosuppression, excessive sweating, the presence of seborrhea, etc. [12, 13]. Complex treatment with local antifungal agents: cream + shampoo (as a shower gel), as well as combination therapy with systemic and local drugs using antifungal shampoo is one way to solve this problem. Along with the main one, at the second stage, preventive maintenance local therapy is required using shampoo 1-2 times a week. [9, 12], mainly after episodes of severe sweating. The establishment of the dependence of the clinical manifestations of mycotic infection on the composition of the sweat-fat mantle has led to the fact that in recent years, shampoo with a combination of zinc pyrithione and ketoconazole has become more actively used in the treatment of patients with Malassezia infection (including pityriasis versicolor) and associated skin diseases [14]. It has been shown that the use of drugs with a sebostatic effect reduces the likelihood of relapses in Malassezia-associated skin diseases [15].
Zinc pyrithione and ketoconazole are included in Keto Plus shampoo (Glenmark Pharmaceuticals Ltd., India). Ketoconazole, like all azoles, inhibits the biosynthesis of ergosterol and has a fungistatic effect in low concentrations, and has a fungicidal effect in higher concentrations - 2%, as in shampoo. Zinc pyrithione has antiseptic, drying, keratoregulating, sebostatic and anti-inflammatory properties. The combined action of the components of Keto Plus shampoo mutually potentiates the effectiveness of therapy. A treatment option has also been proposed, where instead of a 5-day period of use of shampoo, a 2-week period is used, followed by a transition in the case of common forms to preventive use with the application of 1 r./week. for a long period of time in order to increase the reliability of the regimen and reduce the likelihood of relapses [16]. In our practice, we have been using Keto Plus shampoo for the treatment of lichen versicolor since 2009 [17], and during this period we have accumulated sufficient experience in its use both in primary treatment regimens and at the preventive stage. Giving preference to combination regimens using systemic itraconazole (200 mg once a day for 7 days) or an integrated approach using modern topical antifungal drugs in the form of a cream or solution (1-2 times a day for 1-3 weeks. depending on the drug), we almost always, in addition to such treatment, recommend a combination of zinc pyrithione and ketoconazole in the form of shampoo as a shower gel for the entire duration of therapy in the patient’s usual hygienic regimen (optimally 1 time per day). The use of shampoo containing ketoconazole and zinc pyrithione was assessed positively by patients: the texture and smell of the shampoo are pleasant, it foams well, so we began to recommend it instead of cosmetics. In addition, it must be taken into account that most cosmetic shampoos, shower gels and soaps often have a slightly alkaline pH value, and excessive alkalization of the skin creates more favorable living conditions for fungi of the genus Malassezia, which is excluded if replaced with a special Keto Plus product. If the use of shampoo as a drug for treatment in the practice of dermatovenerologists already occupies a worthy place (both in monotherapy and in complex therapy with local antifungal agents), then information about its use for secondary prevention in individuals prone to relapses is rare [16]. We have accumulated sufficient experience in such use, primarily in risk groups: young people who sweat frequently, who are actively involved in physical education and sports, as well as among law enforcement officers who are forced to wear multi-layered warm clothing for a long time. We present the results of our observations. Purpose of the study: to develop approaches to secondary prevention for lichen versicolor in people prone to relapses, using shampoo containing a combination of ketoconazole and zinc pyrithione. Materials and methods: the work was carried out in conditions of predominantly outpatient dermatological appointments in the period from 2011 to 2015. The study included 62 people aged 21 to 36 years, who underwent annual medical examination and had at the time of inclusion at least the second episode of the disease in 3 years, whose skin condition and the occurrence of relapses could be assessed within a period of at least 2 years after the course of combination therapy according to the scheme indicated above. Therapy was continued until complete clinical resolution. Men made up the majority - 55, women were 7 people. The diagnosis before the course of treatment was verified anamnestiically, clinically, Balzer test, laboratory, the clinical form in 45 patients was quite common. HIV infection was excluded in patients. After completion of treatment, it was recommended to use shampoo with a combination of ketoconazole and zinc pyrithione (Keto Plus, Glenmark, India) as a shower gel for prophylactic purposes. Method of application: the shampoo is worn with the formation of foam on wet skin during the shower from the hair to the level of the pelvis, if necessary, lower, and is not washed off for 5-6 minutes, after which the patient is quickly rinsed. The procedure was recommended to be carried out at least 1 time per week, and if episodes of intense sweating occur, even after such episodes, but not more than 3 times per week.
Results and discussion: of the 62 people whose history was tracked during the observation period, 17 patients did not comply with the instructions and stopped using the shampoo immediately after completing the course of therapy. This group was no less interesting than the groups in which patients used Keto Plus shampoo for prevention, and it was assigned the role of a control group. The first group, in which Keto Plus shampoo was used for more than six months but less than a year, included 31 participants. The second group, where patients reported using Keto Plus shampoo for 2 years according to the recommended preventive regimen, included 14 patients.
In the control group that did not receive preventive therapy, relapses at different times during the observation period were noted in 6 (≈35%) people, while common forms of infection reappeared in 2 patients. In the first observation group, in which the period of preventive use of shampoo was from six months to 1 year, no relapses were noted during the period of preventive use of Keto Plus shampoo. The appearance of clinical manifestations of lichen versicolor was observed in 6 patients over a period of at least 8 months. after completing a course of preventive use of shampoo, mainly in the autumn-winter period, they were represented by single typical colonies on the skin of the trunk or neck. The percentage of relapses in the first group was ≈16%, which is more than 2 times less than in the control group. In the second observed group, which used Keto Plus shampoo in the recommended preventive regimen, there were no relapses of the disease continuously throughout the observation period, i.e. for at least 2 years. Patients in this group positively noted the appearance of a large package of shampoo (150 ml instead of 60 ml), which was regarded by patients as an economically advantageous offer, and we, in addition, assessed it as increasing patients’ compliance with the preventive regimen. I would like to note that both during the main course of therapy and during periods of long-term preventive use of Keto Plus shampoo, there were no cases of individual intolerance, either by subjective or objective indicators.
Conclusions: Our observational study clearly demonstrates the effectiveness and safety of a shampoo containing a combination of ketoconazole and zinc pyrithione as a means for secondary prevention of tinea versicolor in the recommended regimen, especially in individuals predisposed to the disease. Unfortunately, the refined contingent of selected patients, small samples and not very long follow-up periods do not allow us to make population-based, statistically based conclusions about the timing of such preventive therapy. We are cautious about recommendations for many years of continuous use of shampoo with a combination of ketoconazole and zinc pyrithione throughout the peak period of the disease, limited, for example, as indicated above, to the age of 40 years. We have formed the opinion that a two-year period of preventive continuous use of Keto plus shampoo in a regimen of at least 1 rub./week, and in the event of episodes of intense sweating - and after such episodes, but not more than 3 rub./week., is quite sufficient for disease control. Based on clinical experience with the use of such a regimen, we can conclude that preventive treatment after the main course of therapy reduces the likelihood of relapses. In some cases, namely, if in some individuals the tendency to relapse of lichen versicolor persists after discontinuation of the prophylactic use of shampoo, it will be more economically profitable to carry out a repeated course of the main treatment, but again with a subsequent repetition of a two-year course of anti-relapse therapy, rather than continuous preventive use throughout the entire peak period of illness.
Thus, in modern conditions, in the arsenal of dermatologists and mycologists there is an effective local component of the treatment of versicolor versicolor in the form of easy-to-use Keto Plus shampoo, which is an etiopathogenetic combination of ketoconazole and zinc pyrithione as a shower gel. It is especially advisable to use it in common, recurrent and atypical forms of the disease, both in combination with systemic drugs and in complex use schemes together with local antifungal creams (solutions) to increase the effectiveness of treatment of lichen versicolor and prevent (reduce the likelihood) of relapses of the disease. In addition, Keto Plus, due to its pronounced antifungal, antiseptic, drying, sebostatic and anti-inflammatory activity, can be recommended for the preventive treatment of lichen versicolor after the main course of treatment 1-2 times per week. lasting up to 24 months. And the unique pharmacological properties of Keto Plus, combined with ease of use, safety (good tolerability) and pleasant organoleptics, give hope for high patient compliance with the prescribed treatment and prevention regimens.
Literature 1. Klimko N.N. Mycoses: diagnosis and treatment. Guide for doctors. 2nd ed. M.: VG Group, 2008. P. 114. 2. Yakovlev A.B., Suvorova K.N. Malassezia is an infection of human skin. Academic method. allowance. M.: GOU DPO RMAPO, 2005. 3. Sergeev A.Yu., Sergeev Yu.V. Fungal infections. Guide for doctors. 2nd ed. M.: BINOM Publishing House, 2008. pp. 230–238. 4. Fitzpatrick T., Johnson R., Wolfe K. et al. Dermatology. Atlas-directory. Per. from English M.: Praktika, 1999. 5. Tarasenko G.N., Tarasenko Yu.G. Fundamentals of practical mycology. M.: OASIS-Design, 2008. pp. 29–34. 6. Abdulloeva M.A., Zoirov P.T. Clinical forms of versicolor versicolor // Healthcare of Tajikistan. 2011. No. 4. pp. 12–15. 7. Arabian R.A., Klimko N.N., Vasiliev N.V. Diagnosis of mycoses. St. Petersburg: Publishing house SPbMAPO, 2004. pp. 60–62. 8. Wolfe K., Johnson R., Surmond D. Dermatology according to Thomas Fitzpatrick. Atlas-directory. Per. from English M.: Praktika, 2007. pp. 834–837. 9. Sergeev Yu.V., Shpigel B.I., Sergeev A.Yu. Pharmacotherapy of mycoses. M.: Medicine for everyone, 2003. pp. 137–138. 10. Dermatovenerology - 2010. Clinical recommendations (Russian Society of Dermatovenerologists) / Ed. A.A. Kubanova. M.: DEX-Press, 2010. pp. 299–301. 11. Wolf K., Goldsmith L.A., Katz S.I. and others. Fitzpatrick’s dermatology in clinical practice: in 3 volumes; lane from English; total ed. A.A. Kubanova. M.: Panfilov Publishing House; BINOMIAL. Knowledge Laboratory, 2012. Vol. 3, 2013. pp. 1995–1998. 12. Ustinov M.V., Sirmais N.S. Systemic therapy of pityriasis versicolor // Polyclinic. 2014. No. 1. P. 80–83. 13. Faergemann J. Pityrosporum infections // J. Am. Acad. Dermatol. 1994. Vol. 31 (Suppl. 1). P. 18–20. 14. Kudryavtseva E.V. Malassezia infections in the practice of a dermatologist // Advances in medical mycology. T.13. M.: National Academy of Mycology, 2014. pp. 118–120. 15. Albanova V.I., Kalinina O.V. Seborrheic dermatitis of the scalp: the role of Malassezia // Advances in medical mycology. T.14. M.: National Academy of Mycology, 2015. pp. 11–13. 16. Abidova Z.M., Shorahmedov Sh.Sh., Alimzhanov D. Study of the clinical effectiveness of ketoconazole shampoo // Advances in medical mycology. T.11. M.: National Academy of Mycology, 2013. pp. 121–123. 17. Ustinov M.V. Treatment of recurrent common forms of lichen versicolor // All-Russian scientific and practical conference “Current issues of dermatology and urogenital pathology”. Abstract. reports. M.: FMBA of Russia, FGOU IPK FMBA of Russia, 2009. pp. 48–50.
Method of infection
Mushrooms can come into contact with the skin of a healthy person, but with strong immunity, the body uses protective functions and the disease does not occur.
Main routes of transmission:
- Skin contact with the carrier.
- In public places: shower, fitting room.
- Use of a person’s personal belongings: towel, washcloth.
When infected with this microorganism, symptoms do not appear for 2 weeks to several months. They may not appear at all unless a situation arises when the immune system weakens.
Symptoms
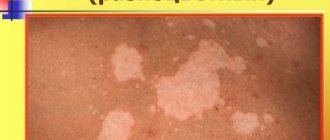
The main symptom of pityriasis versicolor is the appearance on the surface of the skin of asymmetrically located round spots with clear boundaries . They can vary in size and tend to grow larger as the disease progresses. At later stages of pathology, the lesions are characterized by fusion.
The color of such spots is very different and can vary from whitish to pink-red. Layers of small scales are visible on the surface. The skin in these places thickens and changes its structure. The lesions are not characterized by itching or other unpleasant sensations. They do not tan when exposed to ultraviolet radiation and can disappear on their own over time.
Diagnostics
Diagnosis of this pathology is carried out by a dermatovenerologist and is based on objective examination data and additional research methods. Most often, the Balser iodine test is used to clarify the diagnosis. The essence is to stain the spots with a 2% iodine solution, under the influence of which the foci of pityriasis versicolor become colored. The method with an ultraviolet Wood lamp is also used.
Additional examination for the presence of fungi in the layers of the skin is possible.