Acne and more: external signs of liver problems
Acne due to liver disease is a common and understandable problem, but there are other types of skin problems. Redness on the face due to the liver may be of allergic origin. This happens when the body cannot cope with the full processing of, for example, medications. Yellowness and sallowness of the skin are usually caused by excess bilirubin, which is normally excreted by the liver. But these signs usually appear when there are significant health problems. And acne, as the very first marker of problems, breaks out at the slightest problem.
Acne due to the liver is not always a sign of serious pathologies or chronic damage. Rather, on the contrary, a certain number of acne that are resistant to lotions and cleansing simply indicate that the liver needs support, for example, a diet, or giving up some bad habits. Also, acne on the face due to the liver can signal that the medications taken are not suitable for the body.
Dermatological symptoms of liver cirrhosis: the significance of an interdisciplinary problem
The liver of an adult weighs about 1.5 kg. It is covered with a thin, strong connective tissue membrane – Glisson’s capsule [1]. Most of the liver is located on the right side of the body. The liver is projected onto the anterior abdominal wall of the epigastric region. The upper border of the liver normally begins in the 10th intercostal space on the right in the mid-axillary line. From here it rises steeply upward and medially. Along the right nipple line, the liver border can normally reach the 4th intercostal space. Further, the border of the liver descends to the left, crosses the sternum slightly above the base of the xiphoid process, the upper border of the liver reaches the middle of the distance between the left sternum and the left nipple line. The lower border of the liver also begins in the 10th intercostal space on the right, but goes obliquely and medially, crosses the 9th and 10th costal cartilages on the right, runs along the area above the womb obliquely to the left and up, crosses the costal arch at the level of the 7th left costal cartilage and in the 5th intercostal space it connects with the upper border [2]. The location of the inferior border of the liver is one of the most important clinical characteristics of its size. Normally, it is determined below the edge of the costal arch on the right; the protrusion should be no more than 2 cm. The liver consists of 2 main lobes, the right lobe is much larger than the left. The lower surface of the liver is called visceral and is in contact with some parts of the gastrointestinal tract and the right kidney. The upper surface of the liver is smooth, directly adjacent to the diaphragm. On the lower surface of the liver there is a short, deep transverse groove - the porta hepatis. The relative mass fraction of the liver is not the same at different periods of a person’s life: in a newborn, the liver occupies most of the abdominal cavity, and the mass is 1:20 of body weight; in an adult, the weight of the liver is 1:50 of body weight, and its skeletotopy corresponds to that described above [2]. The liver consists of parenchyma formed by hepatocytes and connective tissue stroma. Hepatocytes are functional liver cells that perform at least 500 different functions, from storage (glycogen) to detoxifying (glucuronide). The uniqueness of the liver as an organ also lies in the fact that it is both an exocrine and endocrine gland. The endocrine secretion comes from the liver directly into the bloodstream, and the exocrine secretion is bile. The latter enters the hepatic duct, gall bladder, and duodenum. The common bile duct (ductus choledochus) opens into the duodenum, forming the nipple of Vater. In 1 day, from 0.5 to 1 liter of bile enters the intestine, the dynamics of its intake is determined by digestive need. If there is no such need, bile is deposited in the gallbladder [2]. Bile contains bile pigments (bilirubin), bile salts, proteins, cholesterol, and tissue fluid crystalloids. The main function of bile is to emulsify dietary fats, which is a preparation for enzymatic action. Normally, the amount of bile pigment - bilirubin in the blood is small: its total amount should not exceed 20 µmol/l, and the amount of bilirubin determined by the direct diazoreaction (Jendraszek method) should not exceed 3.4 µmol/l [3]. The latter is a bilirubin glucuronide. The so-called “indirect” bilirubin is a yellow pigment bound to blood proteins that has not been detoxified in the liver. A small amount of toxic “indirect” bilirubin in the blood does not lead to disruption of overall homeostasis. Liver diseases inevitably affect the condition of the skin and its appendages. In this case, symptoms arise, the assessment of which, even in the absence of special studies, makes it possible to make an accurate diagnosis and direct the treatment process in the right direction. One of these serious diseases is cirrhosis of the liver. It is necessary to distinguish between 2 processes, as a result of which the organ loses most of its specific functions. The loss of these functions occurs as a result of the death of specialized organ elements, in this case hepatocytes, and their replacement with connective tissue. These 2 processes are cirrhosis and fibrosis.
Fibrosis is an inactive process, representing scar changes in any organ; once arising, for example, as a result of an abscess, fibrosis fills the missing structure of the organ, although it is functionally untenable. This process does not pose any danger, because it is not active and does not progress. Cirrhosis is an active process of replacement of functionally specialized tissue with connective tissue that no longer performs specialized functions. The main danger of cirrhosis is its steady progression, accompanied by the death of the functional elements of the organ - hepatocytes. The uniqueness of the liver as an organ also lies in the fact that it has pronounced regenerative capabilities and is capable of restoring some of the lost lobules. It is this ability to regenerate that is lost in cirrhosis. Damaged hepatocytes regenerate more slowly than they are replaced by connective tissue. The causes of cirrhosis come down to the action of a number of agents, the activity of which exceeds the adaptive capabilities of the organ [4–6]. The pathogenetic classification of liver cirrhosis is based on the principle of taking into account portal hypertension, the development of cirrhosis as a result of previous necrosis of hepatocytes, and prolonged stagnation of bile. In accordance with this clinical and morphological classification, liver cirrhosis is distinguished: portal, postnecrotic, biliary, mixed. Portal cirrhosis is the most common type of liver cirrhosis (up to 40% of all cases). This species received its name due to the often developing hypertension in the portal vein system of the liver. According to the WHO clinical classification, this is micronodular cirrhosis, and its causes are often alcohol intoxication, fatty hepatosis, pathological conditions with protein-vitamin deficiency; Infectious lesions, for example, Botkin’s disease, may also be important [7]. Another synonym for portal cirrhosis is septal, since it is characterized by the formation of connective tissue septa that fragment the liver lobules. General clinical symptoms of portal cirrhosis include weakness, loss of appetite, pain in the right hypochondrium, alternating constipation and diarrhea, and bloating. The liver is palpable in 85% of cases, the spleen in 40% of cases. Jaundice develops at the beginning of the process in only 12% of patients. An enlarged liver in the early stages of cirrhosis may not manifest itself clinically, and only an increase in the size of the organ indicates trouble. Gradually, the consistency of the liver becomes denser, its surface becomes lumpy, and an increase in size may be replaced by a decrease. Splenomegaly appears later than hepatomegaly [7]. Very quickly, with portal cirrhosis, congestion develops in various venous pools: esophagogastroduodenoscopy reveals varicose veins of the esophagus (from which bleeding is sometimes possible), veins of the anterior abdominal wall (“Medusa’s head”, Fig. 1), and overflow of hemorrhoids [7]. Due to stagnation, the liquid part of the blood plasma leaks into the abdominal cavity, and ascites is formed, sometimes reaching significant sizes. Massive edema develops in the lower extremities. The appearance of ascites always indicates the presence of hepatocellular failure. Indeed, in addition to stagnation, the release of fluid into the tissue is facilitated by disruption of albumin synthesis. This point, combined with sodium retention, leads to a decrease in intravascular colloid osmotic pressure. Sodium retention is due to increased synthesis of aldosterone and decreased inactivation in cirrhosis.
Postnecrotic cirrhosis accounts for up to 30% of all cirrhosis and, according to the WHO classification, corresponds to macronodular cirrhosis. In most cases, this form of cirrhosis occurs as a result of viral hepatitis, as a result of which it is also called “post-hepatitis”. Other causes of this form of cirrhosis are hepatotoxic poisons. Under the influence of all these factors, necrosis of the liver parenchyma occurs, and massive necrosis is followed by collapse of the remaining stroma. The collapsed stroma turns into scars, between which areas of liver tissue are preserved. Since the regenerative ability of the liver is preserved for some time, large nodes of functionally still healthy liver parenchyma are formed between the layers of connective tissue [7]. But, unfortunately, this form of cirrhosis is characterized by rapid progression of the disease, and signs of hepatic cellular failure quickly come to the fore: pain in the right precostal area, dyspeptic disorders. Jaundice develops in most patients and occurs in waves. Astheno-vegetative disorders are often associated. If portal cirrhosis is characterized by slow progression of ascites, then in postnecrotic cirrhosis ascites has a wave-like course and in the early stages can even resolve on its own for some time [7, 8].
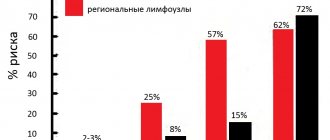
Biliary cirrhosis accounts for 5–10% of all liver cirrhosis. There are primary and secondary biliary cirrhosis. Primary biliary cirrhosis is an inflammatory autoimmune disease of the interlobular and septal bile ducts. The bile ducts are gradually destroyed under the influence of viruses, drugs, and other intoxicants; this condition leads to ductopenia, persistent cholestasis, and progressive liver failure. Thus, the basis of primary biliary cirrhosis is intrahepatic cholestasis. This form of cirrhosis most often affects women aged 40–60 years, the intensive rate is 4–15 cases per 105 people. The average life expectancy of patients with clinical manifestations is 7–10 years [8]. Secondary biliary cirrhosis occurs with cholangitis, congenital defects in the structure of the bile ducts, in the presence of various long-term obstacles to the outflow of bile (stone, scar, neoplasm). Connective tissue develops around the bile canaliculi and along the periphery of the hepatic lobules, resulting in the formation of so-called “false lobules.” Secondary biliary cirrhosis is based on extrahepatic cholestasis. General clinical symptoms of biliary cirrhosis are determined by cholestasis. Characterized by jaundice, itching, steatorrhea, osteoporosis, and bleeding. In clinically pronounced cases, portosystemic encephalopathy develops [8].
Although itching can occur with any liver damage, it is especially painful with biliary cirrhosis. Sometimes its intensity can be compared to the itching of skin lymphoma or severe atopic dermatitis. Itching drives the patient into a frenzy, sometimes to suicide [8]. A distinctive feature of skin itching in liver failure is the presence of only secondary elements - excoriations (scratching), while the primary elements of all kinds of rashes, characteristic of most itchy dermatoses, are absent (Fig. 2). There are no papules, vesicles, tubercles, only sometimes urticaria are found. The functional characteristics of liver cirrhosis of any origin include the following parameters [4, 9]: 1. Hepatocellular failure: – compensated (only changes in stress test parameters, bilirubin level – <34 µmol/l, prothrombin time (PTT) – 1–4 s , albumin level – >35 g/l); – subcompensated (bilirubin level – 35–50 µmol/l, albumin level – 28–35 g/l, PTT – 4–6 s); – decompensated (albumin level – <28 g/l, bilirubin level – > 51 µmol/l, PTT – > 6 s). 2. Portal hypertension: – moderate; – sharply expressed. Cirrhosis is characterized by an intrahepatic form of portal hypertension. 3. Activity of cirrhosis: – inactive; – active (moderate, pronounced). 4. Ascites: – no; - soft; – tense. 5. Encephalopathy: – no; – mild (grade 1–2); – severe (grade 3–4). The death of cells and tissues with such a huge functional set (as already noted, at least 500) that the liver tissue has, determines the whole variety of skin symptoms manifested in a patient with cirrhosis of the liver. Jaundice and itchy skin are essential symptoms of liver cirrhosis. Shades of yellowness can vary widely - from pale yellow to yellow-red. There is even the concept of “subictericity,” when jaundice is subjectively barely discernible; the sign is well defined on the sclera. Jaundice becomes clinically noticeable when bilirubinemia is at least 34–36 μmol/L (2–3 mg%) [1, 9]. The distribution of yellowness over the surface of the skin may be uneven; it is often more pronounced on the trunk and sclera, and to a lesser extent on the extremities. Acute pathology of the hepatobiliary system is often projected in the peri-umbilical zone: with acute cholecystopancreatitis, hemorrhages may appear here, and with a rupture of the common bile duct, a sharp yellow coloration may occur. Mild jaundice occurs in atrophic forms of cirrhosis.
The cardinal symptoms of cirrhosis - jaundice and skin itching - are often accompanied by others that are important not only for verification of the diagnosis, but also for the clinical assessment of the functional state of the liver, the degree of compensation of the pathological process, and therefore for the prognosis. In the therapeutic medical history, the general characteristics of the patient’s skin, as a rule, are not included in a separate status localis. This is one of the initial stages of examining a patient. Portal cirrhosis is characterized by dark pigmentation of the skin, mostly in its exposed areas, which is associated with the deposition of melanin in the dermis; in turn, these melanin deposits are caused by an increased content of estrogens and steroid hormones. There is a so-called sallow complexion. With any form of liver cirrhosis, changes in the hairline occur. Of all the skin appendages, hair is perhaps the most sensitive to intoxication. In patients with liver cirrhosis, a lack of hair in the armpit area can often be found. An increased content of estrogen leads to the fact that even men lose hair in the beard and mustache area and develop gynecomastia [5]. The development of erythema of the palms is a symptom characteristic not only of cirrhosis, but also of any chronic liver disease. However, in cirrhosis, “liver palms” are an integral part of the clinical picture. In addition to erythema, smoothness of thenar and hypothenar is noted. This symptom can be observed not only in patients with liver cirrhosis, but also during pregnancy, rheumatoid polyarthritis, and also in healthy adolescents [5].
The clinical picture of liver cirrhosis is often complemented by various neoplasms. All neoplasms arising against this background are benign. They can be roughly divided into vascular, “storage neoplasms” and hyperkeratotic. Vascular neoplasms include all kinds of hemangiomas, primarily stellate spider-shaped hemangiomas, which are almost as characteristic a sign of liver damage as “liver palms”. They are also called "spiders". They are considered a prognostically unfavorable sign. These “spiders” are localized almost exclusively in the area of the outflow of the superior vena cava: on the forehead, back of the head, shoulders, and the anterior wall of the chest. Morphologically, stellate hemangiomas are punctate, 1–3 mm, ectasia of dark red, cherry-colored vessels. With vitropression, weak pressure with a glass slide, especially when using a dermatoscope, pulsation of the central vessel can be detected. The mechanism of their formation is apparently due to a number of mediators and hormones released during the period of death of hepatocytes. Heparin is one such hormone. In hepatopathy, both arterioles and venules are affected [10]. Spider veins should be differentiated from angioma-like elements in Rendu-Osler-Weber disease (hereditary hemorrhagic telangiectasia), Fabry-Anderson angiokeratoma, Fordyce, and spider nevi. The latter are vascular nevi, exist from early childhood and are not accompanied by pathology of internal organs. Equally harmless is Fordyce angiokeratoma, which is a congenital malformation of the vascular wall. But Fabry–Anderson angiokeratoma requires close attention, because it is a fatal disease [11]. A characteristic but relatively rare symptom of liver cirrhosis is a bluish, crimson or red tongue with severe atrophy of the mucosa and papillae. The lips also become red, as if varnished. This sign is observed in cirrhosis, but is often difficult to interpret and distinguish from other pathological conditions. For example, this sign may be the only manifestation of incipient lichen planus. In addition, atrophy and “varnished” language is often accompanied by candidiasis of the oral mucosa, its atrophic form. Cyanotic tongue, although without pronounced atrophy, can be observed with mitral and mixed heart defects, in which cirrhosis of the liver is not uncommon.
In general, the vascular system is greatly affected by liver cirrhosis. Such patients develop various variants of livedo (Fig. 3) - a kind of dilatation of skin vessels: according to the type of mesh - reticular livedo (livedo reticularis), rings - annular livedo (livedo annillaris), tree crown - tree-shaped livedo (livedo racemosa) [12] . In severe cases, especially at the stage of gradual transition of chronic active hepatitis to cirrhosis, in such patients multiple hemorrhages appear on the skin of the trunk and limbs, and although this condition is called “hepatic purpura,” the nature of the hemorrhages varies from small petechiae to ecchymosis and vibice. If even small-point hemorrhages or hemorrhages in the sclera are detected, it is recommended to perform well-known clinical techniques for assessing the condition of the vascular wall: “tourniquet”, “pinch”, and check for the presence of the Rumpel-Leede symptom. Sometimes the vascular wall suffers so much that hemorrhagic dermographism is detected [12]. Patients may complain of frequent nosebleeds. “Accumulation neoplasms” are represented by xanthomas and xanthelasmas. They are manifestations of functional disorders of lipid metabolism. These neoplasms are not specific to liver cirrhosis and rather indicate a predisposition to lipid deposition in tissues. But since lipid metabolism disorders are an indispensable component of the pathogenesis of liver cirrhosis, the appearance of xanthomas and xanthelasmas is already a clinical component of the clinical and laboratory syndrome of dyslipidemia. Peculiar lipid deposits can form both against the background of hyperlipidemia and in a normolipidemic state. The most common types of cholesterol and lipid deposits in the skin are flat xanthomas and xanthelasmas [13]. They are yellowish-whitish nodules measuring 1 to 5 mm and round or ovoid in shape. Lipid deposition occurs in the upper layers of the dermis, where there is a cluster of foam cells. The cytoplasms of these cells are filled with lipids. Typically, when diagnosing persistent dyslipidemia, multiple flat xanthomas are important.
In addition to flat ones, there are also multiple eruptive xanthomas (Fig. 4), which are larger formations - nodes 5–8 mm in size, painless, scattered throughout the skin; the largest number of them is found on the extensor surfaces of the limbs, back, and buttocks. Often these nodes have an inflammatory rim around the main element [14]. When carrying out differential diagnosis for multiple flat and eruptive xanthomas, one should take into account not only hyperlipidemic and dyslipidemic conditions, but also nosologies that are not directly related to lipid metabolism: these are various hematological diseases, often severe; life-threatening conditions (histiocytosis X, leukemia, myeloma and other systemic diseases). Rarer types of xanthoma are tuberous and tendinous, they do not correlate with liver cirrhosis. Hyperkeratotic neoplasms on the skin in liver cirrhosis can be represented by senile keratomas. These are hyperkeratotic neoplasms of brownish color, 1–2 cm in size, rising above the surface of the skin, dense and rough to the touch. They are localized almost exclusively on the skin of the torso, sometimes located along Langer's tension lines. If there are few of these neoplasms, then they represent an independent nosology and reflect only the tendency of the skin to the appearance of such neoplasms. If, over the course of a year or even a shorter period, a massive burst-like eruption of these keratomas in huge numbers suddenly occurs, then this condition can be regarded as Leser-Trelat syndrome [15], a paraneoplasia caused by gastrointestinal carcinoma. If the number of keratomas slowly increases over 3-4 years, and eventually other symptoms and skin itching join them, then a liver examination is necessary. A specialist can judge a lot by changes in the condition of the patient’s nails. The fact is that another component of the pathogenesis of liver cirrhosis is a violation of protein metabolism, including a violation of keratin synthesis. Often in such patients we find changes in the structure and color of the nails. The endogenous nature of these changes is indicated by their symmetry and multiplicity. For example, single dotted whitish spots on one of the nails of the hands, gradually moving towards the free edge, not only do not indicate the presence of a serious disease, but are not even considered as a pathological condition. To consider the symptom of leukonychia (Fig. 5) as a significant sign, symmetry, multiplicity of changes, as well as a large affected area are required. The most typical for toxic (alcoholic) cirrhosis is total leukonychia - a symptom, although rare, at the same time clearly correlates with the severity of the process [5]. Nonspecific changes in the structure of the nails are much more common: - onychorrhexis - cracks in the free edge of the nail; − onychoschisis – separation of the nail parallel to the horizontal surface; - pinpoint depressions (Rosenau's symptom) similar to psoriatic ones, but in smaller quantities; − longitudinal ridges of nails (like “roof slats”) – found normally in old people, and in young people – with corresponding severe diseases; − hapalonychia (onychomalacia) – a kind of softening of the nail plate due to disturbances in its mineralization; − koilonychia – concave, “spoon-shaped” nails are a variant of hapalonychia, but in combination with other symptoms (subicteric sclera, sallowness of the face, “varnished tongue”) can serve as a criterion for severe intoxication and, accordingly, an unfavorable prognostic sign. Pathology of the vessels of the nail bed is a common occurrence in toxic hepatitis with the outcome in cirrhosis. A splinter symptom is often observed - an expansion of the capillaries of the nail bed and an increase in their permeability, manifested in the form of a thin short “thread” visible through the nail plate (Fig. 6). The appearance of this symptom is a relatively early indication of liver dysfunction, and with cirrhosis this symptom appears regularly.
Hypertrophic lesions of the nails, their excessive compaction (scleronychia), and Hippocratic nails are not typical for cirrhosis of the liver. The classic sign of a long-term drinker has always been facial erythema - a symptom described in many works of fiction. Meanwhile, facial erythema itself, or rosacea, does not directly correlate with the severity of liver damage, but only indicates the fact of alcohol abuse. It is under the influence of alcohol that the blood vessels in the face dilate, which later becomes persistent. However, it is believed that the extreme degree of rosacea - rhinophyma - still correlates in a certain way with the severity of liver damage and can serve as an indicative symptom of established cirrhosis, giving rise to a targeted search. Many of the described skin changes are such indicative symptoms. It is believed that rhinophyma represents the final infiltrative-productive stage of rosacea development. The process can be localized not only in the area of the nose (rhinophyma), but also in the chin (gnathophyma), on the ears (otophyma), and eyelids (blepharophimosis) [15]. Of the 4 types of rhinophyma (glandular, fibrous, fibroangiomatous, actinic), liver cirrhosis is most characterized by the form associated with insolation - actinic. But all of the listed forms of rhinophyma can be observed. Urticaria is a nonspecific syndrome and, in general, is not characteristic of cirrhosis. But it may be one of the signs of active viral hepatitis. In advanced cases of cirrhotic lesions, the appearance of urticaria is caused rather by toxic influences [1, 16].
Thus, all the described symptoms of cirrhotic liver damage can be divided into 2 groups: unconditional and indicative. The unconditional symptoms include the complex “jaundice - skin itching - signs of portal hypertension.” Individually, none of the symptoms is unconditional, but the above complex allows one to suspect cirrhosis. All other symptoms should be considered indicative, in the presence of which an in-depth and targeted study of the liver is indicated. It should also be mentioned about the possibility of the appearance of the 3rd group of symptoms, which are usually referred to as “paraneoplastic dermatosis,” during the transformation of cirrhosis into hepatocellular carcinoma. With the initial appearance of jaundice, patients usually first turn to a therapist and an infectious disease specialist, with severe skin itching - to a dermatologist, and with the appearance of vascular and other neoplasms on the skin - to a cosmetologist. And if in the first 2 cases the patient’s path, as a rule, ends with the establishment of an accurate diagnosis, then for a cosmetologist this path often ends at the stage of removing the cosmetic effect. Thus, all specialists, including cosmetologists, play an important role in the initial tentative diagnosis of liver disease.
Literature 1. Tsirkunov L.P. Skin symptoms in the diagnosis of somatogenic diseases. M.: Znanie-M, 2001. 368 p. 2. Prives M.G., Lysenkov N.K., Bushkovich V.I. Human anatomy. 10th ed. St. Petersburg: Hippocrates, 1997. 704 p. 3. Clinical assessment of laboratory tests / trans. from English / ed. WELL. Titsa. M.: Medicine, 1986. 480 p. 4. Sadovnikova I.I. Liver cirrhosis. Questions of etiology, pathogenesis, clinical picture, diagnosis, treatment // Breast cancer. 2003. T. 5. No. 2. 5. Tischendorf F.V. Diagnosis by external signs. Atlas-handbook of clinical and differential diagnostics / trans. with him. M.: Med. lit., 2008. 320 p. 6. Nam YH et al. Liver cirrhosis as a delayed complication of Stevens-Johnson syndrome // Intern Med. 2011. Vol. 50 (16). R. 1761–1763. Epub 2011 Aug 15. 7. Therapy / trans. from English, revised and additional / ed. acad. RAMS A.G. Chuchalina. M.: GEOTAR-Medicine, 1999. 1026 p. 8. Pinheiro NC et al. Refractory pruritus in primary biliary cirrhosis // BMJ Case Rep. 2013 Nov. 14. 2 013. pii: bcr2013200634. doi: 10.1136/bcr-2013-200634. 9. Lippert G. International system of units (SI) in medicine / trans. with him. M.: Medicine, 1980. 208 p. 10. Silverio AO et al. Are the spider angiomas skin markers of hepatopulmonary syndrome? // Arq Gastroenterol. 2013 Jul-Sep. Vol. 50 (3). R. 175–179. doi: 10.1590/S0004-28032013000200031. 11. Elkin V.D., Mitryukovsky L.S. Selected Dermatology. Rare dermatoses and dermatological syndromes. Handbook of diagnosis and treatment of dermatoses. Perm, 2000. 699 p. 12. Skin pathology. In 2 volumes. Volume 1. General pathology of the skin. / V.G. Akimov, V.I. Albanova, I.I. Bogatyreva and others / ed. V.N. Mordovtseva, G.M. Tsvetkova. M.: Medicine. 1993. 336 p. 13. Rational pharmacotherapy of diseases of the digestive system. Hand. for practicing doctors / V.T. Ivashkin, T.L. Lapina and others / edited by. ed. V.T. Ivashkina. M.: Litterra, 2003. pp. 389–464. 14. Therapist's Handbook / ed. F.I. Komarova. M.: Medicine. 1979. 656 p. 15. Potekaev N.N. Rosacea. M. – St. Petersburg: ZAO “BINOM Publishing House”, “Nevsky Dialect”, 2000. 144 p. 16. Therapeutic Handbook of the University of Washington (series “Foreign Practical Guides to Medicine” No. 1) / ed. M. Wooddy, A. Whelan / trans. from English M.: Praktika, 1995. 832 p.
How it works?
Does the liver affect the skin directly? No, the connection and the mechanism for its implementation are much more complex. The liver, as a natural filter of the body, must transform, bind and remove all toxins, poisons - that is, everything that cannot be removed without additional processing. Since the temperature inside the organ is always higher, the components of almost any poisons disintegrate much faster there into suitable for excretion. But there is a nuance: during the filtration process, the liver itself can become damaged. A simple example is that regular processing of large doses of alcohol disrupts self-healing processes and triggers organ destruction.
A diseased liver “creates” acne in two ways - either the body tries to remove toxins through the skin, and this reduces the immune defense by changing the pH to a more alkaline one. Either more sebum is released through the skin - a little fat is normally excreted through the pores, which in small quantities protects the skin from drying out and helps maintain its elasticity. Increased sebum secretion often indicates problems with the liver: when the skin begins to “shine” 2-3 hours after washing, it’s time to contact a hepatologist. Acne due to liver disease with severe excess secretion of the sebaceous glands is a secondary problem. A large amount of fat is a breeding ground for bacteria and fungi. And if both problems are combined, acne lesions appear with a large number of pimples.
T.V. Dvoryankina: “Skin itching is the lot of not only an allergist, but also a gastroenterologist”
The liver is the main filter of our body, protecting all our organs from the effects of an aggressive external environment. The range of different forms of liver disease is very wide. Among them are non-alcoholic and alcoholic fatty liver disease, chronic viral hepatitis, autoimmune liver diseases, hereditary metabolic liver diseases, cholestatic liver diseases. The latter include primary biliary cirrhosis and primary sclerosing cholangitis, which are less common and therefore the management of these patients is less well known.
We talk about modern methods of diagnosis and treatment of cholestatic liver diseases with the head of the gastroenterology department of City Clinical Hospital No. 12, a doctor of the highest category, Honored Doctor of the Republic of Tatarstan Tatyana Vasilievna Dvoryankina.
— Tatyana Vasilievna, how often do primary biliary cirrhosis (PBC) and primary sclerosing cholangitis (PSC) occur in practice?
— Cholestasis is the basis of cholestatic liver diseases. What is cholestasis? This is stagnation or difficulty in the secretion of bile. It is not an analogue of jaundice, since with it the secretion of bilirubin may not be impaired. It is observed in many diseases of the hepatobiliary zone. Most often in clinical practice, obstructive cholestasis occurs due to cholelithiasis.
Depending on the location, causes and activity, intrahepatic and extrahepatic cholestasis are distinguished. Also distinguished are partial cholestasis (decreased volume of bile secreted), dissociated cholestasis (delayed release of individual components of bile), total (delayed flow of bile into the duodenum).
PBC and PSC are relatively rare diseases. It is believed that per 1 million adults there are 23-50 people with PBC. Among all liver cirrhosis, 6 to 15% are PBC. According to recent epidemiological studies, PBC is common in developed countries. It mainly affects women over 35 years of age.
As for primary sclerosing cholangitis (PSC), it is an autoimmune disease that most often affects men. The average age of patients is 41 years and older.
— What is the etiology of cholestatic liver diseases?
— The etiology depends on the underlying liver pathology. All cholestasis is characterized by the same clinical symptoms: skin itching, acholic stool. Fatigue, weight loss, and dyspeptic pain syndromes are usually associated with the underlying liver pathology.
Itching is a symptom that most clearly indicates possible cholestatic liver disease.
Thus, intrahepatic cholestasis is characterized by a disturbance in the formation of bile acids from cholesterol and the smooth endoplasmic reticulum with a delay in their release. In this case, bile micelles are damaged and bile circulation is disrupted. And extrahepatic cholestasis is associated with a violation of the outflow of bile. How should this problem be solved? If we are talking about stenosis of the duodenal papilla, where the outflow of bile is possible only mechanically, then it is resolved endoscopically. Dissection is performed using special equipment.
Nowadays there are a lot of drug-induced hepatitis that can occur with cholestasis syndrome. In this case, it is important to determine what medications the patient is taking. In particular, in women, the cause of this problem may be the use of contraceptives. They usually proceed very favorably. If we are talking about parenchymal diseases, then even ordinary hepatitis or cirrhosis of the liver can occur with cholestasis syndrome.
In practice, therapists with congenital cholestasis rarely meet. Thus, primary progressive intrahepatic cholestasis (or Beeler's disease) is a hereditary pathology that develops between the ages of 1 and 10 months and is characterized by growth impairment, rickets, and hemorrhagic diathesis. Patients die between the ages of 2 and 15 years from complications of liver cirrhosis.
There is benign cholestasis of pregnancy (idiopathic jaundice). This is a benign familial disease that manifests itself during pregnancy and with its resolution, cholestasis goes away.
All cholestasis show the same type of laboratory data. The first thing that is available is an increase in alkaline phosphatase.
– What modern methods exist for diagnosing cholestatic liver diseases?
– For cholestatic liver diseases, ultrasound is an important tool for assessing the progression of PBC and PSC. Using this method, you can see the presence of stones in the gall bladder, the width of the common bile duct, and the size of the pancreas. Computed tomography (CT) and magnetic resonance imaging, both with and without contrast, are used to exclude intra- and extrahepatic tumors, as well as to assess the condition of the biliary tract. Ultrasound and CT are necessary to exclude tumors and pathology of the bile ducts.
Endoscopic examinations are also carried out. Duodenoscopy is used when the area of the duodenal papilla is examined. If inflammatory diseases, strictures, the presence of diverticula or tumors are detected, surgical treatment is prescribed.
Previously, radioisotope diagnostics were very widely used. The method of duodenal intubation has not lost its relevance. For the diagnosis of diffuse liver diseases such as cirrhosis and hepatitis, the gold standard is a needle biopsy.
In Kazan, laboratories carry out a wide range of hematological, general clinical, biochemical, serological, immunological, bacteriological and other types of research.
The first biochemical change indicating the possible presence of PBC or PSC is an increase in the level of alkaline phosphatase, bilirubin, and the determination of antimitochondrial antibodies.
Detection of antimitochondrial antibodies most reliably indicates the presence of PBC and practically excludes PSC and other cholestatic diseases. Antimitochondrial antibodies are detected in almost 100% of patients with PBC.
– Do antioxidants and hepatoprotectors play any role in the treatment of liver diseases?
– Antioxidant stress is the basis of any pathology. The theory is that the formation of free radicals causes cell damage. Today there are about six groups of hepatoprotectors.
Each drug has its own niche. Each patient should be approached individually and, based on the symptoms, the drug should be prescribed. Herbal preparations are widely used. Which includes milk thistle.
— What mistakes do doctors make when diagnosing PBC or PCC?
— As I already said, the main symptom of cholestasis is itchy skin. Therefore, patients first go to dermatologists or allergists. If the patient is 35 years old and has itchy skin, then she should be referred for consultation to a gastroenterologist. Treatment should be carried out in collaboration with a therapist and doctors of other specialties. There is an increase in patients suffering from liver diseases worldwide. In our country, great importance is given to cardiovascular pathology. But, unfortunately, young doctors have gaps in the diagnosis and treatment of liver pathology.
I would like to note one more aspect. With cholelithiasis, stones do not develop immediately. It is important to monitor risk groups and hereditary factors. First of all, a primary care doctor should focus on prevention. And now even young women who want to lose weight diligently exhaust themselves with hunger and various fasting diets form gallstones. If there is a tendency to stone formation, then fasting is contraindicated! One of the important tasks of a doctor is to set the patient up to lead a healthy lifestyle and proper nutrition.
Gulnara Abdukaeva
Restore skin clarity
Clear facial skin is not a luxury; everyone wants to get rid of suddenly appearing acne. Moreover, they are often painful. However, if skin problems are caused by liver pathologies, you will have to try to get rid of acne:
- change your diet by removing gifted, fatty, smoked, sweet, spicy foods
- give up alcoholic, low-alcohol and non-alcoholic carbonated drinks
- If you are following a “fat burning” diet, reconsider your diet in favor of a balanced diet
- if there is a need to take medications that seriously damage the liver, discuss with your doctor how to neutralize the harm
- drink more clean water
- carry out a “general cleaning” of the body and cleanse the liver using detoxifying drugs
The relationship between “removing acne and cleaning the liver” has been known for a long time; this connection was known even in ancient times. Natural hepatoprotectors of plant origin were already popular among both ordinary and noble people, since the quality of nutrition seriously affected the liver and acne. The relationship between clear skin and an abundance of cabbage, turnips, greens and fermented milk products in the diet was tracked by doctors who put patients with liver disease on some kind of diet - there was no talk about the beauty of the skin. However, along with the pain, heaviness in the right hypochondrium and nausea, the rashes on the face disappeared.
In more advanced cases, decoctions and infusions of milk thistle, sage, calamus, and mint were used - natural hepatoprotectors, which, together with diet, gave a pronounced effect. This liver cleansing removed acne even faster and better, and the general condition of the body became much better. Actually, one of the most effective pieces of advice from cosmetologists is still this: the best way to get rid of acne is to cleanse the liver.
Using a diet for cleansing is reasonable and safe, but you still shouldn’t use old recipes for infusions. Instead of herbal preparations with dangerous side effects and allergies, it is better to use modern hepatoprotectors, which include exclusively necessary active ingredients. The best option is to use hepatoprotectors based on silymarin, an active substance isolated from milk thistle. The drug Legalon, containing silymarin of the highest degree of purification, is completely free of all the side effects that are caused by an unrefined decoction of the plant. It allows you to safely cleanse the liver, and the skin gradually returns to normal.
What foods should you not eat if you have acne?
Not only smoking and alcohol, but also some everyday foods can cause intoxication of the body and deterioration of the skin. They affect the level of glucose and cholesterol in the blood, thereby enhancing the functioning of the sebaceous glands. The body strives to remove the resulting toxins out, which leads to the appearance of acne.
According to the results of a number of studies, in regions where the population consumes a minimum amount of animal fats, the incidence of acne is below the world average. This proves the effectiveness of prescribing a diet for illness.
What foods to avoid for acne? When treating acne, you should avoid the following products:
- Sweets. Sugar and refined foods (for example, refined flour) provoke the accumulation of insulin, which leads to the production of male hormones - androgens. All this provokes increased production of sebum, which clogs the pores. When bacteria attach, acne appears.
- Dairy products. Traditionally, milk is considered a healthy product, but it is really only necessary for children. Adults lose the ability to digest cow protein, which causes an increase in insulin in the blood. Betacullin contained in milk causes the growth of new cells and slows down the death of old ones, which is not normal. The worst dairy products that cause acne are full-fat cheese and whey-based milkshakes, which act like concentrated milk.
- Flour products, porridges (cereals, boiled porridges), pasta, starchy foods. Cereals (wheat, rye, barley) and products based on them contain gluten in large quantities. This substance forms gluten, which interferes with normal intestinal function. Products based on wheat flour and starch cause the release of insulin, which provokes the appearance of acne.
- Coffee. This drink stimulates the production of cortisol, the stress hormone. It has a destructive effect on the liver and causes an increase in blood sugar.
- Fast food, semi-finished products and sauces. Foods that should not be eaten if you have acne include those that contain flavor enhancers and trans fats (snacks, hamburgers, chips, onion rings). They cause not only addiction and the growth of adipose tissue, but also the formation of acne on the skin.
- Alcohol. Alcohol-containing drinks dilate blood vessels, causing redness of the skin and dehydration.
- Fat meat. Dishes made from foods containing animal fats enhance the work of the sebaceous glands, which subsequently provokes the appearance of acne.
Some products, deservedly classified as healthy and dietary, can provoke acne:
- Spinach. The vegetable is an excellent source of iron. At the same time, spinach contains iodine, which, when accumulated in the body in large quantities, can provoke the appearance of imperfections on the skin.
- Peanut. This is a healthy product, but not for those suffering from acne, since these nuts contain a substance that enhances the production of sebum.
Safety precautions: how to avoid relapse
Cleansing the liver and facial skin are connected, and the opposite effect in the form of the return of acne at the slightest problem with filtering toxins occurs constantly. How to prevent acne from returning after cleansing? There are several ways:
- once and for all formulate a diet that excludes foods harmful to the liver;
- give up alcohol - all organs will be grateful, not just the liver;
- give up strict diets that provoke fatty hepatosis;
- monitor your immunity, promptly treat all colds and infectious diseases;
- take hepatoprotectors in preventive courses as needed;
- drink more clean water;
- regularly breathe fresh and clean air in parks or gardens, preferably outside the city.
Quite simple tips that, unlike the strict prohibitions of a chronic patient, can be violated occasionally - one fried pie every couple of months will most likely not cause acne. And the best part: the rules can be supplemented with your own observations, because each organism is unique.
It is important to remember that acne resistant to cosmetic procedures and the liver have a very direct connection. Therefore, if suddenly acne and oily skin become a problem, you need to make an appointment with a hepatologist. Just in case.
Liver and skin diseases
Skin and liver diseases are in many cases closely related, and there are a number of reasons for this.
Firstly, they have common risk factors: alcohol abuse, excess weight, fat metabolism disorders (increased blood cholesterol levels), carbohydrate metabolism disorders (increased blood glucose levels, diabetes mellitus).
Secondly, the inflammatory process plays a central role in the development of many liver and skin diseases. Moreover, some inflammatory reactions have a common mechanism.
Thirdly, skin diseases can become systemic (widespread) in nature, that is, involve other organs. The liver is one of the most commonly affected skin diseases.
And finally, fourthly, if there are signs of liver disease, the skin disease is often characterized by a more severe course and is more difficult to treat.
One of these diseases, the development, course and effectiveness of treatment of which largely depends on the condition of the liver, is psoriasis.
Psoriasis, or psoriatic disease, is a chronic skin disease (dermatosis) characterized by excessive division of cells in the surface layer of the skin (epidermis), disruption of normal keratinization of the skin and inflammation, as well as involvement of various organs.
The development and progression of psoriasis, in addition to heredity, stress, smoking and infections, is also facilitated by disease risk factors - alcohol abuse, impaired metabolism of fats and carbohydrates, excess weight.
Diagnosing psoriasis is usually not difficult. It is characterized by the formation on the skin of flat pink papules (nodules) with a rough surface, covered with silvery-white scales that can be easily removed. Any area of the skin can be affected, but more often the extensor surfaces of the limbs, the sacral area and the scalp. Also, in the diagnosis of psoriasis, the PASI (the Psoriasis Area and Severity Index) index of psoriasis coverage and severity can be used - a calculated index based on an assessment of the area affected by various parts of the body (head, torso, arms and legs). To assess the quality of life, a special questionnaire is used - the dermatological life quality index DLQI (Dermatology life quality index).
Liver damage in psoriasis occurs due to immune mechanisms, when inflammation no longer becomes local, only in the skin, but widespread in the body (psoriatic disease).
In addition, drugs for systemic treatment of psoriasis (taken orally, administered intramuscularly or intravenously) often have hepatotoxic effects and can cause drug-induced liver disease (DLD).
On the other hand, the presence of any liver disease in psoriasis plays the role of an additional aggravating factor.
A sign of liver dysfunction in psoriasis associated with one reason or another is an increase in the level of liver enzymes - ALT (alanine aminotransferase) and AST (aspartate aminotransferase).
Thus, complex treatment of psoriasis cannot always be limited to external medications. For the treatment and prevention of liver diseases associated with widespread psoriatic process and/or the use of systemic medications, hepatoprotectors may be required.
A hepatoprotector that can stop inflammation not only in the liver, but also in the skin, that is, it also has a dermoprotective effect, is the drug Phosphogliv*.
Phosphogliv* take 2 capsules 3 times a day with meals, without chewing, with a small amount of liquid. The duration of the course is 3-6 months.
If you suspect psoriasis and concomitant liver disease, you should consult a doctor.
Bakulev A.L., Shtoda Yu.M., Utz S.R. On the issue of comorbidity in psoriasis. Saratov scientific and medical journal. - 2014. - No. 10 (3). – P. 537–539.1
Butov Yu.S., Vasenova V.Yu., Shmakova A.S. and others. Clinical and biochemical status in patients with psoriasis and methods of its correction. Ross Journal of Skin and Vein Bol. – 2009. – No. 5. – P. 23—27.2
Emchenko Ya.A. Features of the clinical course of psoriasis in patients with concomitant metabolic syndrome depending on the level of systemic inflammation // Medical news of Georgia. – 2014. – No. 11 (236). – P. 43-46.3
Korsunskaya I.M., Dvoryankova E.V. et al. Features of the treatment of psoriasis in patients with chronic viral hepatitis // Russian Journal of Skin and Venereal Diseases. - 2007. - No. 1. - P. 36-39.4
Kochergin N. G. Psoriasis: modern ideas and prospects // Med. messenger – 2007. – No. 5. – P. 9-10.5
Kubanova AA Psoriasis. Clinical recommendations / Ed. AA Kubanova. Russian Society of Dermatovenerologists. – M.: DEX-Press, 2008. – 56 p.6
Kubanova A.A., Martynov A.A. Clinical and economic analysis as a new paradigm of dermatovenereology // Bulletin of dermatol. and venerol. – 2005. – No. 3. – P. 25-28.7
Kubanova A.A., Kubanov A.A., Nicholas J.F. et al. Immune mechanisms of psoriasis. New strategies for biological therapy // Vestn Dermatol i Venerol 2010; 1: 35—47.8
Skripkin Yu.K., Kubanova A.A., Akimov V.G. Skin and venereal diseases // Textbook. – 2011. – 544 p.9
Tkachenko S. G., Kondrashova V. B. Cardiometabolic risk in patients with psoriasis. Dermatology and venereology. – 2010. No. 48 (2). – P. 11–16.10
Yakubovich A.I. Correction of lipid metabolism disorders in patients with psoriasis // Ross Journal of Skin and Vein Bol. – 2011. – No. 6. – P. 29—32.11
Augustin M. Co-morbidity and Age-related Prevalence of Psoriasis: Analysis of Health Insurance Data in Germany // Acta Derm. Venereol. 2010; 90: 147-151.12
Barker JWN Pathogenesis and clinical features of psoriasis // Lancet. 2007; 370: 263—271.13
Krueger JG The role of Th 1 – cell in the pathogenesis of psoriasis // 20th World Congress of Dermatology. Paris, 2002. – Book 1.14
Lowes MA, Suarez-Farinas M, Krueger JG Immunology of psoriasis // Annu. Rev. Immunol. 2014; 32: 227—255.15
Ma C, Harskamp CT, Armstrong EJ et al. The association between psoriasis and dyslipidaemia: a systematic review // Br. J. Dermatol. 2013; 168(3):486–495.16
Mallbris L., Granath F., Hamsten A. et al. Psoriasis is associated with lipid abnormalities at the onset of skin desease // J Am Acad Dermatol. 2005; 54: 614-621.17
Nestle FO A large scale genetic association study confirms IL12B and leads to the identification of IL23R as psoriasis - risk genes // Am. J.Hum. Genet. 2007; 80: 273-290.18
Nestle FO, Kaplan DH, Barker J. Psoriasis // N. Engl. J. Med. 2009; 361:496-509.19
Reich K. The concept of psoriasis as a systematic inflammation: implications of disease management // JEADV. 2012; 26 (2): 3-11.20
Ryan C., Korman NJ, Gelfand JM Research gaps in psoriasis: opportunities for future studies // J Am Acad Dermatol. 2014: 70 (1): 146—167.21
Späh F. Inflammation I atherosclerosis and psoriasis: common pathogenic mechanisms and the potential for an integrated treatment approach // Br J Dermatol. 2008; 159 (2): 10-17.22
Wu Y. Prevalence of cardiovascular risk factors and other comorbidities among psoriasis patients // J Am Acad Dermatol. 2007; 191(9):23-27.23