A dysplastic nevus is a pigmented formation that has characteristic clinical and histological features that distinguish it from a noncellular nevus. Dysplastic nevus, which occurs in 5-9% of the white population [1, 2], has recently attracted the attention of researchers, as it may be a precursor to superficial spreading melanoma: it is found in almost all patients with hereditary melanoma and in 30-50% patients with sporadic melanoma [1]. Dysplastic nevus can occur on intact skin or be a component of a complex noncellular nevus [1, 3].
Dysplastic nevi were first described in 1978 by W. Clark et al. [3]. When examining patients with hereditary melanoma and their relatives, the authors identified special pigmented formations that histologically consisted of atypical melanocytic hyperplasia, lymphoid infiltration, tender fibroplasia and newly formed blood vessels that occur in a mixed nevus or de
novo
. The authors explain that the term melanocytic hyperplasia is synonymous with melanocytic dysplasia, when individual melanocytes or small groups of them have some structural features of malignant melanocytes, the development trend of which is not yet clear. W. Clark et al. draw an analogy with cervical dysplasia, when foci of epithelial cells have signs of malignancy, but can remain indolent, regress or progress to overt cancer.
The term dysplastic nevus was proposed by D. Elder et al. [4], who, continuing the research of W. Clark, identified nevi with melanocytic dysplasia in patients with non-hereditary, i.e., sporadic melanoma. The authors designated this phenomenon as “dysplastic nevus syndrome.” They found two morphological types of intraepidermal melanocyte growth disorder in patients with this syndrome: the most common type, lentiginous melanocytic dysplasia (LMD), was observed in all dysplastic formations and resembled the changes occurring in lentigo simplex
, which is reflected in the name “lentiginous”. A second type of growth disorder, epithelioid cell melanocytic dysplasia, was found in two lesions in addition to lentiginous dysplasia. This pattern of growth resembled classic superficial spreading melanoma.
In 1982 Z.V. Golbert, professor at the Moscow Research Institute P.A. Herzen, regarding LMD as a variant of Dubreuil’s melanosis, similar to the stages of development of this disease, identified three degrees of development of LMD [5]. In grade I, there was an increase in the number of melanocytes in the basal layer of the epidermis and some atypia (atypia of location, increase in size, enlargement of the nucleus, hyperchromia, nuclear polymorphism were noted in individual cells). In grade II, there was a more pronounced proliferation of melanocytes, in some places completely replacing the basal row of keratinocytes, and an increase in signs of their anaplasia. This stage is characterized by the presence of elongated acanthotic cords and the tendency of melanocytes to gather in groups and clusters, especially in the acanthotic cords, which created their flask-shaped thickening. The latter structures are especially characteristic of stage III LMD: there was a tendency for melanocytes to grow into the higher layers of the epidermis, as well as for atypical melanocytes to grow deeper into the papillary layer of the dermis. This picture approximates that of melanoma in situ
.
A similar dysplastic nevus was discovered in 2005 by M. Sachdeva et al. [6]: they described a lesion that does not fit into the classic picture of a dysplastic nevus, but does not yet have sufficient evidence for melanoma in situ .
Z.V. Golbert et al. [5] noted that with LMD, as well as with Dubreuil’s melanosis, from the very beginning of the proliferation of melanocytes, even without noticeable signs of their atypia and anaplasia, there is a reactive lymphoplasma cell infiltration and angiomatosis at the base of the dermis. The similarity of the morphological picture of dysplastic nevus and lentigo maligna (Dubrey's melanosis) was also revealed by F. Farrarhi et al. [7].
Clinically, dysplastic nevus is similar to borderline nevus, but there are also differences [1, 2, 8-10]. Thus, a dysplastic nevus is an irregularly shaped spot, while a borderline nevus has a regular shape - round or oval. The color of a dysplastic nevus is often heterogeneous, with areas of dark pigment, while a borderline nevus is characterized by a uniform color, the color of both nevi varies from light brown to dark brown. Often, a punctate formation resembling a target is noted in the center of a dysplastic nevus [9]. When dysplastic and mixed nevi are combined, there is a picture of “fried eggs” with a raised yolk in the center [2]. Noncellular nevi appear in childhood or adolescence, go through stages of development from borderline to mixed and intradermal, and in old age they lose pigment and become fibrotic. Dysplastic nevi appear throughout life, from adolescence to old age, remain dormant for a long time or disappear, and fibrosis is not typical for them [1, 2]. A. Mindy [2] reports that 20% of patients with dysplastic nevi over 50 years of age noted the appearance of new pigmented formations in adulthood.
The final diagnosis of dysplastic nevus is established by histological examination. Due to certain difficulties in the differential diagnosis of noncellular nevus and LMD, the study should be carried out by a pathologist with experience in diagnosing melanocytic formations.
In our observations, dysplastic nevi were found in 5-10% of patients who consulted a surgeon or oncologist for various diseases. In some, the nevi were single (from 3 to 10 formations), in others they were multiple (from 50 to 100 or more). Observing patients with multiple dysplastic nevi, we identified two types of these formations.
In the first type (there were fewer such patients), dysplastic nevi appeared in childhood and adolescence and were often hereditary, but these patients did not report melanoma in relatives. Carriers of nevi were, as a rule, white-skinned, poorly tanned, with blond or red hair and light eyes. Dysplastic nevi of this type were large (0.5-1.0 cm in diameter), located on open and closed areas of the body (buttocks, lower abdomen), and were often combined with papillomatous nevi. The color of nevi in the same patient could vary from pink to dark brown, sometimes a variegated color was observed: dark areas on a pink or light brown background. A similar picture of nevi was described by W. Clark et al. [3] as B-K
mole
syndrome and D. Elder et al. [4] as “dysplastic nevus syndrome”. After puberty, new nevi did not appear in this group of patients. This fact can be attributed to the fact that white-skinned people limited their exposure to the sun, as they quickly burned, and were also informed about the possible appearance of new “moles” as a result of exposure to ultraviolet radiation.
In the second type, dysplastic nevi in adolescence were rare; most nevi appeared in adulthood and were associated with frequent and prolonged exposure to the sun while vacationing in southern latitudes. Dysplastic nevi of this type were small (from 0.1 to 0.4 cm in diameter), regular rounded in shape, uniform in color, combined with multiple freckles in young patients and pigment spots such as Dubreuil’s melanosis in older patients. In white-skinned patients with skin phototype I-II, the nevi were light brown, in others they were brown or dark brown. The density of nevi was higher on sun-exposed areas of the body: on the face, forearms, outer surface of the shoulders, upper back and chest wall (like a “wide neckline”). M. Sachdeva et al. [6], observing 75 patients with dysplastic nevi that arose de
novo
, also noted that in 73 patients the nevi were located on sun-exposed areas of the body. All this indicates some similarity between dysplastic nevi of the second type and Dubreuil’s melanosis, which is a proliferation of melanocytes in the basal layer of the epidermis in individuals with skin phototype I-II under the influence of repeated sunburn.
Dysplastic nevus - what is it?
Like most moles in humans, a dysplastic (atypical) nevus is a pigmented nevus consisting of nevus cells. These cells are very similar to melanocytes. They also secrete the brown pigment “melanin”, but they differ in a number of characteristics that are not of fundamental importance to us.
It is important to note that dysplastic nevus is a histological diagnosis. This means that not all moles that look dysplastic in appearance will actually turn out to be dysplastic after removal and examination.
Treatment
The main surgical treatment is removal of the nevus.
Indications for removal
- heredity for melanoma
- signs of transition of Clark's nevus to melanoma
If a patient has a lot of atypical nevi, then all of them should not be removed. What to do? To observe such a patient, once every six months a dermatologist takes photographs of skin areas with nevi. At subsequent appointments, he compares photographs. If growth is noted, such formations should be removed.
If the operation cannot be performed due to the patient’s serious condition, wipes moistened with fluorouracil or other antitumor drugs (cytostatics) can be applied.
The operation is performed under local anesthesia. And only with a scalpel. Not used: laser (more about laser removal), radio wave (more about the radio wave method of treatment) and other devices.
The spot itself and 3 mm of healthy skin around it are removed, since atypical cancer cells can spread over such a distance around. At the end of the operation, a cosmetic atraumatic suture is applied.
Forecast
Depends on the stage and heredity. In most cases, the prognosis is favorable.
Information for doctors
According to recent studies in the USA, dysplastic nevus is actually a type of typical melanocytic nevus. And in this benign stage, if it does not grow, does not show signs of malignancy into melanoma, it should not be removed. It is only necessary to continue clinical observation of such a patient, especially if there is a family history.
How to distinguish a regular mole from a dysplastic nevus?
Atypical nevi have a number of characteristic features that can occur either individually or in combination with each other.
| Round, symmetrical shape | Uneven edge and/or asymmetrical shape |
| Completely flat or completely raised above the skin | One part can be raised, the other flat (fried egg) |
| Uniform color or shades of brown | Black, red, brown at the same time |
| Size less than 6mm | Size over 6mm |
| Localization on any part of the body | Rarely located on the face |
Links[edit]
- "Melanoma". www.clevelandclinicmeded.com
. - ^ a b James, William D.; Berger, Timothy J.; and others. (2006). Andrews' diseases of the skin: clinical dermatology
. Saunders Elsevier. ISBN 978-0-7216-2921-6. - ^ ab Tchaikovsky, R., FAMMM syndrome: pathogenesis and treatment
, Dermatological Surgery, Vol. 30 Issue 2 p. 2, pp. 291-296, 2004 - ^ ab «FAMMM: In familial cancer syndromes. D. L. Riegert-Johnson et al. NCBI 2009". Retrieved July 21, 2009.
- Silva JH, Sá BC, Avila AL, Landman G, Duprat Net JP (2011). "Atypical mole syndrome and dysplastic nevi: identification of risk groups for the development of melanoma - review article". Clinics (Sao Paulo)
.
66
(3):493–9. DOI: 10.1590/s1807-59322011000300023. PMC 3072014. PMID 21552679. - "FAMMM: In familial cancer syndromes. D. L. Riegert-Johnson et al. NCBI 2009". Retrieved July 21, 2009.
How to distinguish a dysplastic nevus from melanoma?
A theoretically prepared reader, after reading the table, will exclaim: “You have now listed almost all the symptoms of melanoma!!! How can you tell them apart???” Unfortunately, a person without experience in diagnosing skin cancer, as a rule, cannot do this.
If you find moles on your skin with signs of dysplastic nevi, you need to see an oncologist. This doctor will examine them and also tell you about the signs of nevi turning into melanoma and the principles of monitoring such formations.
Diagnosis
It is determined by a dermatologist according to dermatoscopy (examination through a magnifying glass). If necessary, additional examination: dermatobiopsy and histological examination.
Most often, a correct diagnosis can be made based on dermatoscopy data, especially if there is evidence of melanoma (malignant nevus).
Clark's nevus on dermatoscopy
On video: case from practice No. 3. Watch from 2 minutes and 34 seconds. A woman has signs of Clark's nevus turning into melanoma.
It should be differentiated: with borderline nevus, with fibroepithelial nevus, with basal cell carcinoma and melanoma.
Dysplastic nevus syndrome
Unfortunately, there is a syndrome that in Russian literature is often called nevus dysplastic syndrome (in foreign literature - FAMMM).
This disease has 2 diagnostic criteria
- the number of dysplastic nevi on the skin is more than 50
- melanoma in relatives
This disease may be associated with a mutation in the CDKN2A gene, which also increases the risk of developing pancreatic cancer
With this syndrome, the risk of developing melanoma, according to different authors, varies from 56 to 100%. The disease requires regular (once every few months) monitoring by an oncologist.
Clinical manifestations
In most cases, it is not difficult to determine the specific type of nevoid skin formations after a detailed examination of them.
The following features of their appearance may suggest the idea of dysplastic nevi:
- They acquire their atypical appearance from the moment of their appearance;
- They can be either isolated or spread over the entire surface of the skin;
- Most actively appear in puberty and young people
The appearance of dysplastic nevi is presented in the table:
| Quantity | From 1-2 to 100 or more |
| Favorite localization | Mainly arms and upper torso |
| Dimensions | Always large (about a centimeter) |
| Coloring | Contains pigment elements with colors of varying intensity (from light light pigmentation to rich brown). Characteristic is the alternation of areas of different intensity within one nevus |
| Elevation above the surface of the skin | Protrudes slightly above the surface of the skin or is at its level |
| Surface | It's never smooth. It is characterized by a finely tuberous structure, reinforced in the central sections, especially with elevated types of nevi. Peripheral sections are less elevated and smooth |
| Form | Most often irregular, edges uneven and fuzzy |
| Additional signs | Very often there is a growth of pathological hairs from the nevus (black, long, thick) |
What to do if there are dysplastic nevi on the skin?
There is an opinion on the Internet that “all dysplastic nevi should be removed.” I consider this point of view incorrect for the following reasons:
- A very small percentage of nevi that look atypical upon examination turn out to be so upon histological examination.
- An even smaller proportion (0.0001%) of truly dysplastic nevi have a chance of becoming melanoma
- Skin melanoma can develop not from a nevus, but against the background of unchanged skin.
In this regard, for people who have dysplastic nevi, I usually recommend the following:
- Regular self-examination once a month with measurement of existing atypical nevi using a ruler. Optimally - with photographic recording of the result
- Examination by an oncologist once every 6 or 12 months. The frequency depends on the number of nevi.
- It makes sense to remove elements that are difficult to access for self-examination, as well as those that have changed in a short time
- Protect skin from the sun
results
Of the 82 removed pigmented formations, the clinical diagnosis of dysplastic nevus was confirmed morphologically in 62 cases, i.e., LMD structures were found in these formations during histological examination. In 2 cases, melanoma was detected that developed against the background of LMD, in 7 - intradermal nevus, in 10 - mixed nevus, in one - nevus of the sebaceous glands.
Morphologically verified dysplastic nevi and two melanomas were removed from 45 patients (in some individuals, 2-3 nevi). The distribution of patients by age was as follows: 20-29 years - 11 people, 30-39 years - 18, 40-49 years - 9, 50-59 years - 1, 60-69 years - 6. Melanoma was identified in women 49 and 30 years. In total there were 36 women, 9 men. The population of the clinic consists mainly of young and mature people, most of them are female, which was reflected in the gender and age composition of the patients. Some authors [10], however, note that melanoma is the most common malignant tumor in women 25-29 years old.
The removed dysplastic nevi were small in size: 0.3 cm in 3 cases, 0.4 cm in 11 cases, 0.5 cm in 10 cases, 0.6 cm in 5 cases, 0.7 cm in 13 cases, 0.8 cm - in 4, 1.0–1.5 cm in diameter - in 16 cases. Melanoma in 1 case had dimensions of 0.5×0.4 cm, in another - 0.5 cm. As can be seen from the data presented, dysplastic nevi 0.5 cm or less were noted in 24 cases. Foreign authors [1, 2, 10] recommend removing dysplastic nevi measuring 0.6 cm or more; according to our studies, smaller nevi (0.4–0.5 cm in diameter) should also be removed.
Most of the removed dysplastic nevi were localized on the trunk, of which 21 were on the abdominal wall, 7 in the upper back, 7 in the lumbar region. Fewer nevi were located on the chest wall - 4, below the shoulder blades - 1, in the sacrum - 2. There were two nevi in the groin area, 10 on the lower limb, 7 on the upper limb, and 1 on the neck. The melanoma was localized on the forearm and chest wall.
Considering the distribution of dysplastic nevi on the body, it can be assumed that on vacation in hot countries, the upper back, chest, abdominal wall and lumbar region are exposed to intense solar radiation.
In a histological study of 62 dysplastic nevi, LMD that developed de
novo
was found in 24 cases; in 38 cases, there was a combination of LMD with a mixed, intradermal or borderline nevus (see table). Our studies are consistent with the data of other authors, who note that dysplastic nevi in the majority are complex nevi with components of a borderline and intradermal nevus [5, 6, 9]. In two of our cases, melanoma was also detected against the background of a mixed nevus.
The degree of development of lentiginous melanocytic dysplasia identified during histological examination of removed dysplastic nevi.
As can be seen from the table, LMD of II-III degree was identified in 20 formations, i.e. in these cases there was a progressive dysplastic nevus.
Analyzing the clinical signs of 20 progressive dysplastic nevi (with histological signs of stage II-III LMD) and two melanomas, we identified some features that distinguish them from nevi with mild (I and I-II) degree of dysplasia.
According to our observations, the most important sign of the progression of a dysplastic nevus is the appearance of a pigmented formation on unchanged skin and its further growth over several months or years in people over 18 years of age, i.e. in adulthood. Changes in the last 3-5 years of a long-existing nevus may indicate the progression of a dysplastic nevus, which is combined with a borderline or mixed nevus.
An important sign of a progressive dysplastic nevus is a very dark color (almost black) or uneven coloration of the formation with areas of dark brown or black. The irregular shape of the nevus may be little noticeable with a small size of the progressive dysplastic nevus, but at the same time it can also be observed in a long-existing noncellular nevus - borderline or mixed.
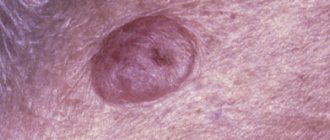
In Fig. Figure 1 shows a dysplastic nevus without signs of progression, 0.6×0.5 cm in size, light brown in color, with a characteristic “target” in the center. According to histological examination, stage I-II LMD.
Rice. 1. Dysplastic nevus without signs of progression. According to histological examination, stage I-II LMD.
In Fig. Figure 2 shows a dysplastic nevus measuring 1.0×0.4 cm, also without signs of progression: oval in shape, with smooth contours, dark brown in color. According to histological examination - mixed pigmented nevus with foci of stage I LMD.
Rice. 2. Dysplastic nevus without signs of progression. According to histological examination - mixed pigmented nevus with foci of stage I LMD.
In Fig. Figure 3 shows a nevus of the chest wall in a 27-year-old patient, 0.3 cm in diameter, round in shape, which darkened after staying in the south (a sign of progression). According to histological examination, mixed dysplastic pigmented nevus with severe LMD (grade III).
Rice. 3. Dysplastic nevus with signs of progression. According to histological examination - mixed dysplastic pigmented nevus with severe melanocytic lentiginous dysplasia (grade III).
In Fig. Figure 4 shows a nevus of the gluteal region measuring 0.5×0.4 cm in a 29-year-old patient with skin phototype I. The nevus, according to the patient, appeared 7 months ago in the form of a punctate formation, which gradually increased in size (a sign of progression). No other pigmented nevi or freckles were found on the body. According to histological examination, lentiginous pigmented nevus with severe LMD (grade III).
Rice. 4. Dysplastic nevus with signs of progression.
Progressive dysplastic nevi require excision for the purpose of prevention, as well as early diagnosis of skin melanoma. When melanoma is detected, the question of the need for reoperation (excision of the postoperative scar) is decided depending on the thickness of the tumor, determined by histological examination. According to foreign authors, as well as WHO recommendations, an adequate deviation from the boundaries of the formation for melanoma in
situ
is 0.2-0.5 cm, for invasive melanoma with a thickness of less than 1.5 mm - 1.0 cm [12].
In our observations, in a case where melanoma in
situ
, the formation was excised at a distance of 0.4 cm, so reoperation was not required. The patient has been observed for 5 years without recurrence of the disease. In the second case, in a 30-year-old patient with a clinical diagnosis of dysplastic nevus of the chest wall, the formation was excised at a distance of 1.0 cm from the visible boundaries. Histological examination revealed melanoma with a thickness of less than 0.75 mm, Clark invasion level - 2, reoperation was also not possible required.
Diagnostics
The following help differentiate Clark's nevus from other skin neoplasms:
- Dermatoscopy. As part of this method, the mole is examined under multiple magnification. Dermatoscopy is effective in detecting melanoma at an early stage of development.
- Indication isotope . Used for early detection of melanoma. With such a tumor, the process of phosphorus absorption by the body is accelerated.
- Echography. It is prescribed to determine the exact location and depth of germination of skin tumors.
- Thermometry. Malignant neoplasms are characterized by a rise in temperature in the area where the tumor is located. Thermometry allows us to identify such changes.
- Radiography. During this procedure, carried out using specialized equipment, it is possible to evaluate the structure of the skin tumor and identify the presence of seals.
Sometimes, for age spots on the body, a biopsy is prescribed. More often, the method is used after removal of the tumor. This is explained by the fact that during a biopsy the integrity of the nevus is disrupted, which can lead to serious complications.
Causes
Melanocytes (cells that synthesize melanin) are located in the layers of the epidermis. This pigment protects the skin from the negative effects of ultraviolet radiation.
What happens if you scratch a mole
Moles (nevi) are formations that appear on the human body in childhood.
Under normal conditions, melanin is evenly distributed throughout the layers of the epidermis. But in people with a genetic predisposition to the formation of moles, melanocytes are concentrated in certain areas, which contributes to the appearance of Clark nevi.
The process of formation of age spots does not depend on human actions. The area in which moles form is determined at the stage of fetal development. This explains the reason why nevi occur in children in the first years of life.
In the future, the appearance of pigment spots is caused by the influence of external or internal factors. The first is ultraviolet radiation.
Prolonged exposure to sunlight triggers mutations responsible for the appearance of nevi. In some people, age spots occur due to the activity of certain viruses (in particular, the human papillomavirus). The influence of this factor stimulates the division of melanocytes.
In addition, the likelihood of nevus formation is directly related to hormonal status. Women often develop new birthmarks during pregnancy. Some relationship has also been identified between the state of immunity and the appearance of nevi.
Advantages of histological diagnosis in Israel
- Diagnostics are carried out by highly qualified specialists with extensive clinical experience.
- Testing is carried out promptly, within 1–3 days.
- During histological evaluation of the material, additional criteria are applied that are not used in medical institutions of the CIS countries.
- Remote examination of material samples is possible.
- Pathological laboratories in Israel have the necessary certificates for conducting any tissue research, incl. genetic.
Melanoma is easily curable in the initial stages and is actually curable even at the stage of micrometastasis - a timely and correct diagnosis is crucial.
Sources
- https://www.cancernetwork.com/articles/histology-melanoma-and-other-skin-cancers
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1770634/
- https://www.slideshare.net/raghuramchary50/histopathology-of-malignant-melanoma