Lichen planus is a chronic disease, prone to relapse, which is accompanied by itchy skin and inflammatory rashes in the form of purple papules.
This disease often affects the mucous membranes of the mouth or genitals. According to WHO, lichen planus accounts for about 2.5% of all dermatological diseases and 15% of diseases of the oral mucosa.
The complex of diseases that make up lichen planus includes two syndromes: Little-Lassuere syndrome, including non-scarring alopecia of the armpits and pubis and scarring alopecia of the scalp, as well as Grinshpan-Potekaev syndrome, including diabetes, hypertension and an erosive-ulcerative form of the dermatological disease.
The exact cause of the pathology is unknown. There are neurogenic, viral, bacterial, autoimmune and toxic-allergic theories of the nature of the disease.
There are a number of factors that increase the likelihood of developing lichen planus, namely:
- genetic predisposition;
- nervous system disorders;
- failure of immunity;
- allergic (lichenoid) reactions to chemical or food components;
- chronic infections in the body;
- metabolic disorders;
- stress;
- injuries to the skin and oral mucosa (presence of sharp edges of teeth, poorly made dentures);
- changes in the microelement composition of saliva due to the presence of dentures made of different metals in the oral cavity;
- aggressive effect of certain medications;
- age after 40 years, etc.
Treatment of this disease is complex and requires an individual approach. Based on the test results, the doctor selects a regimen and dosage of drugs, usually of local action, which reduce the symptoms of the pathology and prevent its reappearance.
What is lichen planus?
Lichen planus is an inflammatory dermatosis with various clinical manifestations. The pathological process involves skin tissue and its appendages (nails and hair), as well as mucous membranes. Usually the disease affects representatives of both sexes of middle and older age, but sometimes it is observed in children.
In modern medicine, it is believed that lichen planus is a delayed-type hypersensitivity reaction in response to the action of a neoantigen of epidermal (skin) origin, since the autoimmune aspect has a significant place in the nature of the disease. Cytokines released by immune cells provoke cytotoxic mechanisms and trigger cell death (apoptosis).
Lichen planus is characterized by three stages:
- progressive, which is accompanied by the active manifestation of symptoms of the pathology: the formation of papules and itching;
- stationary with a gradual decrease in signs of the disease: pallor, flattening of papules and subsidence of itching;
- regressive, which is characterized by regression of papules, the formation of brown spots and areas of atrophy at the site of their localization, and the disappearance of itching.
A little anatomy
The pharynx is part of the respiratory tract and digestive tract. It contains a whole complex of lymphoid formations called the Pirogov-Waldeyer pharyngeal ring. The ring includes the palatine, pharyngeal, lingual, tubal tonsils, as well as lymphoid granules and ridges that are located on the lateral walls of the pharynx.
The tissues of the pharynx are penetrated by a huge number of blood vessels. Their superficial location provides warming or cooling of the air inhaled through the mouth and nose. In contact with the mucous membrane, the air is cleared of dust, chemical impurities and various microorganisms. Dust particles, substances and microbes settled on the mucous membrane irritate it, which sometimes causes inflammation and redness of the throat1.
Up to contents
How to identify lichen planus?
The external manifestation of lichen planus is caused by the processes of damage and regeneration of skin cells and mucous membranes.
The following symptoms are characteristic of lichen planus:
- the presence of polygonal, flat-topped, colored papules 1-2 mm in diameter;
- grouping of papules with the formation of rings or lines;
- the formation of large plaques from papules (Wilham stack), along the periphery of which isolated small papules are located;
- symmetrical localization on the skin (wrist joints, forearms, legs, genitals, etc.);
- the appearance of neoplasms on the inside of the cheeks, gums, tongue, red border of the lips or genitals when the mucous membrane is damaged;
- thinning, brittleness, clouding of the nail plates;
- pronounced itching;
- rapid appearance of papules due to skin injuries (Koebner phenomenon);
- formation of secondary hyperpigmentation in place of the disappeared papule.
Doctors classify the main morphological forms of lichen planus as:
- typical, most common (45% of cases) form of pathology, accompanied by the formation of pearl-colored papules with a specific coating;
- hyperkeratotic or verrucous, characterized by the formation of hard red, gray-yellow or dark red infiltrated plaques on the front of the leg or upper limbs;
- exudative-hyperemic (25% of cases), causing the formation of edematous papules;
- erosive-ulcerative, often resulting from exudative-hyperemic lichen and accompanied by the formation of small ulcers or areas of erosion on the feet or in the interdigital space, etc.
Also in some cases, rare bullous, atypical and pigmented forms of the disease are observed.
The appearance of the first signs of the disease requires immediate medical response. Lack of timely treatment can lead to rapid progression of the pathology and a significant weakening of the body's defenses. What tests are done for lichen planus?
Typically, the diagnosis of lichen planus includes:
- blood test (general and biochemical);
- hormonal profile;
- scraping for histological and cytomorphological examination (affected tissues are susceptible to hyperkeratosis, degeneration of the epidermis, the presence of infiltrate, etc.);
- skin biopsy;
- consultation with a dentist and other related specialists (endocrinologist, gastroenterologist).
When visiting a doctor, it is extremely important to provide him with a list of medications taken, episodes of recent dental treatment, vaccination or viral disease. History data will greatly help in making the correct diagnosis and determining the nature of the origin of lichen planus.
Causes of red throat
Redness of the throat may be due to factors unrelated to infection2:
- Mechanical injuries to the mucous membrane of the pharynx due to solid food and bones.
- Eating hot food that can cause thermal burn2.
- Irritation or burn of the pharynx with chemicals (acids, alkalis, alcohol-containing liquids)2.
- Eating excessively spicy foods (hot pepper, ginger, horseradish, mustard can cause irritation of the mucous membranes).
- Inhalation of tobacco smoke, dust or air contaminated with mechanical and chemical impurities.
Eating food containing red food dyes. In this case, the throat is red, but does not hurt.
Up to contents
How dangerous is lichen planus?
Lack of treatment or a severe stage of the disease can lead to damage to the entire skin, severe discomfort and a significant decrease in immunity.
Lichen planus on the scalp can cause irreversible hair loss, and on the nail plates - nail deformation (thinning, splitting, rejection of the nail plate, even nail lysis).
A pathological lesion in the eye area can lead to blurred vision or narrowing of the tear duct.
The erosive form of the disease often leads to the formation of scars, and the result of lesions of the genital mucosa can be narrowing of the vagina or phimosis.
Also, some forms of the disease are prone to malignancy and degeneration into squamous cell skin cancer.
Traditional Treatments
Key Points
- Traditional medications used for LP include topical and systemic corticosteroids, phototherapy, retinoids, topical calcineurin inhibitors, and systemic immunosuppressive drugs.
- Lesions of the mucous membrane of the oral cavity, genitals, and the follicular form of LP do not tend to spontaneously resolve and often require systemic therapy.
- To date, an insufficient number of clinical studies have been conducted on the treatment of LP. Lack of data does not always indicate the lack of effectiveness of a treatment method.
LP is an important and understudied clinical problem. Thus, the evidence base for the large number of treatment options widely used in clinical practice remains inadequate. Next, the basics of pharmacology and the evidence base for each drug used in routine practice will be discussed, separately for the most common variants of the disease in clinical practice. A brief overview of traditionally used drugs, their pharmacodynamics and level of evidence is given in Tables 1-5.
Cutaneous form of LP
Topical and systemic corticosteroids
The goal of therapy for the classic self-limited cutaneous form of LP is to accelerate the process of resolution of the lesion, as well as symptomatic relief of itching. The standard first-line therapy is topical corticosteroids, and the choice of drug in most cases is based on the clinical experience of the physician rather than on clinical trial data. Commonly used drugs include clobetasol propionate, fluocinolone acetonide, betamethasone dipropionate, triamcinolone acetonide (can also be used as intralesional injections in cases of hypertrophic LP that are refractory to treatment). The authors recommend the use of ointment bases, as they have more pronounced moisturizing properties, as well as a less complex composition compared to creams. TGCS applications are used for lesions up to 15% of the body area; for more extensive lesions, in some cases it is preferable to use systemic drugs. Systemic corticosteroids, both for oral and intramuscular use, can be used for forms of LP that are resistant to topical corticosteroids. The most commonly used is prednisolone at a dose of 30-60 mg/day; the duration of therapy depends on the severity and refractoriness of the disease. A placebo-controlled randomized clinical trial showed that patients refractory to topical corticosteroids experienced significant improvement with a 10-day course of systemic prednisolone at a dose of 30 mg/day. For severe cases of LP, the course duration is up to 4-6 weeks. It is necessary to remember the side effects of systemic corticosteroids, especially when prescribing drugs of this group for a long period. Long-term monitoring of blood pressure and urine glucosuria levels is necessary. Repeated courses of systemic corticosteroids should be avoided whenever possible. A thorough examination of the patient is mandatory to detect symptoms of long-term use and toxicity of systemic corticosteroids using appropriate diagnostic methods. The mechanism of action of systemic GCS is rather nonspecific, based on the induction of immunosuppression and an anti-inflammatory effect, realized through the regulation of the action of proinflammatory mediators at the genetic, cytokine and cellular level. The lack of specificity of pharmacological action leads to a number of side effects, so further research is needed to find a targeted drug.
Phototherapy, photochemotherapy
Phototherapy and photochemotherapy have been used for many years in the treatment of inflammatory dermatoses, including LP, due to their complex immunosuppressive effects. Recent randomized controlled trials show the superiority of phototherapy over treatment with systemic corticosteroids; In a study of patients with TGCS-refractory disease, a 6-week course of narrowband UV-B phototherapy was associated with a complete response in 52% of patients, while a response was observed in 13% of patients with systemic prednisolone therapy for the same duration (however, prednisolone was used in a dose less than the standard one). According to a retrospective cohort study, narrowband UVB phototherapy and PUVA (psoralen+UVA phototherapy) have comparable clinical efficacy in the classic cutaneous form of LP, however, it is preferable to use narrowband UVB phototherapy, since the method is simpler and has a more acceptable safety profile.
Retinoids
Retinoids have been used long-term to successfully treat cutaneous LP, with acitretin being the most commonly prescribed drug. It is believed that the pharmacological effects of acitretin are realized through the activation of retinoic acid receptors, which control the maturation of the epidermis and the inflammatory response in the skin. A double-blind, placebo-controlled study of patients with cutaneous LP showed that an 8-week course of acitretin at a dose of 30 mg/day is associated with long-term remission of the disease. However, a higher incidence of side effects has been reported in patients treated with acitretin, which explains the lack of widespread use of acitretin and other systemic retinoids in patients with cutaneous LP. Other studies have shown the clinical effectiveness of other systemic retinoids - etretinate, isotretionin, tretinoin, however, the indications for the use of drugs in routine practice are limited.
How to cure lichen planus?
The composition and tactics of treatment for lichen planus depend on the degree of spread of the lesion, on the cause and localization of the pathology, on information about the effectiveness of previously administered therapy. Thus, treatment of the disease involves the use of systemic and external medications, as well as phototherapy.
Among the most effective medicinal groups of drugs for the treatment of lichen planus, experts identify:
- antihistamines;
- multivitamin complexes;
- antifungal agents;
- systemic corticosteroids;
- systemic retinoids, etc.
Damage to the oral mucosa in LLP
Topical and systemic corticosteroids
Topical corticosteroids are first-line drugs for the treatment of localized forms of LP of the oral mucosa. Strong and very strong drugs - clobetasol, triamcinolone, betamethasone, fluocytonide, fluticasone - have proven effectiveness and safety. These drugs are usually applied 2 times a day, either undiluted (eg clobetasol propionate 0.05%) or mixed with Orabase (eg triamcinolone) for 1-2 months, followed by maintenance use. It is also possible to use GCS in the form of intralesional injections, but there is insufficient data to support the advantage of this method over others (there are only isolated clinical cases). Systemic therapy using oral corticosteroids may be indicated in case of significant severity of the disease, in case of refractory to external therapy, however, the evidence base for this approach is insufficient; adequate placebo-controlled studies have not been conducted. Taking into account the wide range of side effects associated with the use of systemic corticosteroids, this group of drugs is used in the form of a short course with subsequent transition to topical therapy.
Topical calcineurin inhibitors
Interest in the possibility of using topical calcineurin inhibitors was attracted primarily by their anti-inflammatory effect, which is different from tGCs. The mechanism of action of the drugs is realized by suppressing the activity of T cells at the level of transcription factors. Published studies examining the effectiveness of this group of drugs are very contradictory - a meta-analysis performed in 2012, evaluating 3 randomized controlled trials, showed that the effectiveness of pimecrolimus was no greater than placebo. Subsequent studies were more encouraging - according to the data obtained, the effectiveness of topical calcineurin inhibitors was comparable to the effect of tGCs. A 2014 study found that pimecrolimus was slightly more effective than tacrolimus, while more recent studies found that tacrolimus and pimecrolimus were equivalent. These data were confirmed in an open randomized controlled trial (2017), a pilot randomized controlled trial, and a subsequent meta-analysis. Many physicians have found tacrolimus to be more effective in their clinical practice. Side effects of topical calcineurin inhibitors include local irritation and burning, especially on eroded lesions (which limits their use in the case of the erosive form of LP), but in general their safety profile is not inferior to long-term use of corticosteroids. The absence of side effects of TGCS determines increasing interest in the use of these drugs in clinical practice.
Topical and systemic retinoids
Retinoids have certain immunomodulatory effects due to their direct effects on T cells through nuclear retinoic acid receptors. Topical retinoids are an alternative to corticosteroids for non-erosive LP and are recommended as a second-line drug according to World Workshop in Oral Medicine IV. Despite the proven effectiveness of topical tretinoin and isotretinoin 0.1% (in placebo-controlled studies), one study showed lower effectiveness compared to tGCs. Side effects include local irritation, photosensitivity, and teratogenicity. The possibility of disease relapse within 2-5 weeks after stopping use of the drug significantly limits the widespread use of topical retinoids in everyday practice. The use of systemic retinoids (etretinate, isotretinoin) is limited due to an insufficient risk-benefit ratio, however, the use of alitretinoin may be more successful.
Clinical observation
Patient S., born in 1978, was admitted to the skin department of the Kirov Regional Clinical Dermatovenerologic Dispensary on February 18, 2019 with complaints of rashes on the skin of the upper and lower extremities. Skin itching occasionally bothers me. Reduced quality of life.
Considers himself sick for 2 years, when rashes appeared on the skin of the front surface of the legs. The onset of the disease is not associated with anything. There is no hereditary history of skin diseases. I did not treat myself, nor did I see a doctor. Later, the number of rashes increased: new elements appeared on the skin of the upper and lower extremities, and skin itching intensified. He was treated on an outpatient basis: local ointment with betamethasone. The last exacerbation occurred within 2 months, when I noticed the appearance of new rashes on the skin of the thighs and forearms. I contacted a dermatologist at my place of residence.
Anamnesis of life.
Born in the Kirov region. Education: secondary specialized, pedagogical. Denies HIV, tuberculosis, hepatitis A, B, C, blood transfusions, and previous sexually transmitted infections. Denies drug intolerance. Previous diseases: acute respiratory diseases, sore throat. There is no hereditary history of skin diseases. Denies injuries or surgeries. Denies chronic diseases. Denies bad habits.
General inspection.
The condition is satisfactory, consciousness is clear. When examined using the methods of auscultation, palpation and percussion: the internal organs are unremarkable. Heart rate 76 beats/min. Blood pressure 120/70 mm Hg. Art. Physiological functions are normal.
Local status.
The pathological process on the skin is widespread, symmetrical, chronic in the acute stage. Localized on the skin of the upper extremities (in the area of the shoulders, forearms), lower extremities (in the area of the thighs, legs, ankles, dorsum of the feet). It is represented by multiple papular elements of pink color with a purple tint, 0.2–0.5 cm in diameter, polygonal in shape, with an umbilical depression in the center. Some papules merge, forming rings with a slight depression in the center with a diameter of up to 3.0 cm (Fig. 1–3). When illuminated from the side there is a waxy sheen. Wickham's grid sign +. Dermographism is mixed. Peripheral lymph nodes are not enlarged.
Data from the conducted research.
Clinical blood test: leukocytes 3.3×109/l; red blood cells 4.62×1012/l; hemoglobin 140 g/l; platelets 337×109/l; erythrocyte sedimentation rate 6 mm/h; eosinophils 2%; lymphocytes 1.0×109/l. General urine analysis: straw-yellow, transparent; protein 0.017 g/l; specific gravity 1.025; glucose: negative; pH 6.5; leukocytes and erythrocytes were not detected. Biochemical blood test: alanine aminotransferase 53 U/l; aspartate aminotransferase 32 U/l; cholesterol 5.03 mmol/l; total bilirubin 10.9 nmol/l, glucose 6.0 mmol/l.
HLA phenotype: A02, 28, B07, 18. DRB1* 04.
Ultrasound of the abdominal organs from 02/20/2019: inflection of the gallbladder.
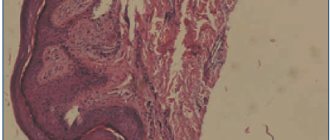
The result of the biopsy: epidermis of uneven thickness, focal hyperkeratosis, focal hypergranulosis, foci of vacuolar degeneration. In the dermis there is swelling of collagen fibers, collapsed vessels. In the superficial layers of the dermis there is a band-like lymphohistiocytic infiltrate (Fig. 4).
Treatment
the patient was prescribed in accordance with the standard of specialized medical care for LLP. The dose of prednisolone was prescribed: 30 mg/day intramuscularly No. 3, then the tablet form 20 mg/day (in the morning) with a gradual reduction in the dose after discharge by 1/2 tablet once every 10 days until complete withdrawal and subsequent administration of hydroxychloroquine. As replacement and concomitant therapy, including for the prevention of side effects, the patient received omeprazole, antihistamines, potassium preparations, calcium gluconate, vitamins A and E, ferrous sulfate and vitamin C. Local treatment: mometasone furoate.
The duration of treatment in hospital is 14 days. The patient was discharged with complete resolution of the elements, with some remaining hyperpigmentation under dispensary observation by a dermatovenerologist at his place of residence.