In this article we will tell you:
- What can a chemical burn be like?
- How to understand what exactly got into your eyes?
- The first signs of a chemical burn to the eyes
- First aid for chemical burns
- Why is it necessary to go to the doctor after a chemical burn to the eyes?
- How to assess the degree of eye damage from a chemical burn?
- How are patients with chemical eye burns treated?
- How to prevent eye burns?
Chemical burns to the eyes account for about 10% of eye injuries for which people consult doctors. And since this happens so often, everyone should know how to properly provide first aid for a chemical burn to the eyes.
Most of them happen at work, for example, in industries where they work with chemicals. Chemical burns also often occur in the home from cleaning products or other common household products. They can also be very dangerous and cause irreparable damage to the organ of vision, they must be treated seriously and immediately.
What can a chemical burn be like?
- Alkaline. This is the most dangerous type of chemical injury to the eye - alkali dissolves the tissue of the eye and penetrates deep into it. The higher its concentration, the faster necrosis occurs. Possible if ammonia bleach, cleaner, lime, cement or magnesium comes into contact with eyes;
- Acidic. It is caused by vinegar, acetone, peeling solutions or glass polish. Typically, with such a burn, only the cornea is affected. But concentrated hydrofluoric or sulfuric acid can melt tissue right down to the lens. Damage to the cornea itself can also cause loss of vision - a thorn appears on the eye;
- From other irritants, such as pepper spray.
Symptoms
Symptoms of a chemical burn depend on the concentration of the substance.
If an accident occurs with acid up to 9%, which is most often used in everyday life, you can hope for a favorable outcome.
But
70% vinegar can completely melt the cornea and lead to the formation of a cataract, which cannot be treated.
When vinegar gets on the cornea, a person experiences :
- severe burning and pain;
- tearfulness;
- itching;
- dizziness.
These symptoms include blurred vision and redness of the eyes and eyelids.
How to understand what exactly got into your eyes?
In order not to waste precious time finding out the cause, it is better to consult a doctor as soon as possible. It is very difficult to visually determine what caused the burn. For example, if there are crusts, one can only assume that acid has gotten into the eyes, but in reality it is difficult to see them. Everything is complicated by the fact that due to the reflex, the eyelids are tightly closed during a burn. Therefore, the conclusion is usually made based on what the person has worked with. If the victim has used ammonia bleaches, cleaners, lime, cement or magnesium, this is definitely an alkaline injury.
Consequences
Even a small amount of vinegar that gets on the cornea does not pose a direct threat to the health of the victim .
A chemical can cause damage to the eye even without symptoms: this is the insidiousness of a burn.
Reference! Acid concentration of 1-9% leads to burns of the first degree, 70-90% - moderate and severe.
In severe cases, the acid burns through the cornea to the sclera , resulting in the formation of a fairly large white spot.
Because of it, vision becomes blurred or almost completely lost .
Complete or partial clouding of the lens leads to irreversible pathological changes in the ocular structures.
Their consequence is complete loss of vision.
The most harmless consequence of a vinegar burn is infection of the mucous membranes . In this case, a course of antibacterial treatment will be required.
First aid for chemical burns:
❗ Do not try to wash off acids with alkali and vice versa - this can only worsen the damage. Also, do not rinse with water if lime or superglue gets into your eyes. According to experts, treating a combined corneal burn is much more difficult. Try to see a doctor as soon as possible for examination and treatment.
❗ Regardless of the type of chemical burn to the eyes, the first thing to do is to carefully open the eyelids and thoroughly rinse the eyes from the outer edge to the inner. This can be done using a rubber bulb, a pipette, a syringe without a needle, or simply with your palms. The same procedure is performed for thermal burns.
❗ It is best to wash your eyes with purified or boiled water, but running water (12-18°C) will also do. You can bend over and put your eye under the faucet. The procedure time is at least 20 minutes. This is necessary in order to reduce the concentration of the substance. After you have washed the substance from the victim’s eyes, you can drip a 4-5% solution of lidocaine, novocaine or another anesthetic and take a pain reliever.
❗ If a powdery chemical gets into your eyes, remove its remnants from your eyes with a dry cotton swab before rinsing.
Publications in the media
Chemical burns of the eye are one of the emergency conditions in ophthalmology that can cause impaired or complete loss of vision. Frequency. 300 cases/100,000 population (burns with alkalis account for 40% of all cases of eye burns, with acids - 10%). The predominant age is 18–65 years. The predominant gender is male.
Etiology • Alkalis •• Ammonium hydroxide (ammonia) – NH4OH •• Sodium hydroxide – NaOH •• Magnesium hydroxide – Mg(OH)2 •• Potassium hydroxide – KOH •• Calcium hydroxide (slaked lime) – Ca(OH)2 • Acids •• Hydrochloric acid - HCl •• Hydrofluoric acid - HF •• Acetic acid - CH3COOH •• Sulfuric acid - H2SO4.
Risk factors • Construction work • Use of chemicals in everyday life (ammonia, aggressive cleaning agents) • Working with car batteries (contain concentrated sulfuric acid as an electrolyte) • Use of concentrated acids and alkalis in production technology • Alcoholism. Pathomorphology • Overflow of capillaries with blood is the morphological substrate of hyperemia • When exposed to alkali - hydrolysis of cell membranes, leading to cell death. Pathological changes are quite widespread • When exposed to concentrated acids - the formation of a scab of denatured proteins. There are practically no pathological changes under the scab • Precipitation of glycosaminoglycans, causing clouding of the cornea • The effect of cations on collagen leads to hydration, thickening, shortening of collagen fibers.
Differentiation of acid burns from alkali burns •• With acid burns, protein denaturation occurs and a scab is formed, which prevents the acid from spreading deeper into the tissue. Damage, as a rule, is limited to the eyelids, conjunctiva, cornea •• In case of burns caused by exposure to alkali, hydrolysis of proteins occurs, a scab does not form, so the alkali penetrates deep enough into the tissues, causing, among other things, damage to the eyelids, conjunctiva, cornea, sclera, lens and even retina. Alkali burns are considered much more dangerous than acid burns, since in the initial stages the depth and area of damage seem insignificant, but subsequently increase significantly. The severity of burns depends on the concentration of the chemical and on the timing and adequacy of emergency care. The full area of burns can be determined only after 48–72 hours.
Classification and clinical picture depending on the severity. • I degree (mild) •• Pain and blurred vision •• Hyperemia and swelling of the skin of the eyelids, conjunctiva (including chemosis) •• Mild clouding of the moisture of the anterior chamber. • II degree (medium) •• Pain syndrome and decreased visual acuity. With alkali burns, the pain is more pronounced immediately after alkali gets into the eye, then the pain becomes less intense •• Formation of blisters surrounded by a halo of hyperemia on the skin of the eyelids, erosion of the conjunctiva, corneal epithelium with the formation of easily removable films, ciliary injection. • III degree (severe) •• Necrosis of the skin of the eyelids, formation of difficult-to-remove films on the conjunctiva, severe clouding of the cornea (“ground glass”) •• Significant chemosis and pallor of the conjunctiva (ischemia of the perilimbal region) •• Cloudiness of the aqueous humor of the anterior chamber of the eye. • IV degree (very severe) •• Widespread necrosis of the skin, conjunctiva and sclera •• Chemosis and ischemia of the perilimbal region •• Cloudiness of the cornea is so intense that it resembles a porcelain plate •• Cloudiness of the aqueous humor of the anterior chamber of the eye •• Increased IOP •• Local necrotizing retinopathy. • Burns of the III and IV degrees leave behind pronounced changes - ulcerative defects that heal with the formation of scars of both the conjunctiva and cornea (cataract), fusion between the conjunctiva of the sclera and the eyelids (symblepharon).
Research methods • Study of visual acuity • Tonometry • Fluorescein staining to identify ulcerative defects of the cornea • Biomicroscopy to determine the condition of the anterior part of the eye • Ophthalmoscopy to identify changes in the fundus.
TREATMENT Mode . Providing first aid at the scene of the incident, then hospitalization is indicated. For mild burns caused by non-concentrated acids, it is permissible to limit yourself to only consulting an ophthalmologist. Management tactics • First aid •• Eye rinsing should be carried out no later than 30 minutes after a chemical substance gets into the eye •• Washing should be done with 200–300 ml of 0.9% sodium chloride solution or weak (1:5000) potassium solution permanganate. Flushing with water is also possible in an emergency situation. Washing with neutralizing solutions is not recommended, since the formation of reaction products between alkali and acid with an unpredictable effect on damaged barriers is possible. For lime burns, it is possible to instill a 5% EDTA solution into the conjunctival sac, which forms a soluble, easily washed out complex with calcium compounds •• Introducing a local anesthetic into the conjunctival cavity in a solution or ointment (for example, 0.5% tetracaine solution) • • Mechanical removal of settled particles of the chemical substance •• Administration of antitetanus serum according to Bezredka (3000 IU).
• Treatment in a hospital •• Long-term use of local anesthetics should be avoided. They can be replaced with codeine 30–40 mg orally •• Cycloplegics (1% atropine solution or 0.25% scopolamine solution 2 times a day in eye drops) - to reduce pain and prevent the formation of intraocular adhesions •• Antibiotics locally to prevent infection, for example, tetracycline eye ointment every 2–4 hours, eye drops with ciprofloxacin every 2–4 hours •• Tear substitutes, for example, natural tears every 4 hours •• To reduce IOP when it increases - topical timolol 0.5 % solution 2 times a day, and/or orally acetazolamide 125–250 mg orally every 6 hours, and/or mannitol 20% solution 1–2 g/kg IV •• GC for intraocular inflammation: prednisolone 1 % or equivalent every 1–4 hours for 10–14 days; for severe lesions - prednisolone 20–60 mg orally 4 times a day for 5–7 days. If the epithelium is damaged, quickly cancel it.
Surgical treatment • Puncture of the anterior chamber to remove chemical reagents from the eye cavity • Tarsorrhaphy (temporary stitching of the eyelids) for persistent epithelial defects • Tissue replantation in case of threatened or acute perforation of the cornea • To restore the germinal layer of the epithelium - transplantation of an autograft of the conjunctiva or limbus • Layer-by-layer or penetrating keratoplasty in the presence of corneal scars.
Complications • Iridocyclitis • Corneal ulcers with subsequent formation of a cataract • Corneal perforation • Progressive symblepharon and entropion • Neurotrophic keratitis • Glaucoma • Cataract • Eye hypotonia • Fibrovascular pannus • Destruction of the eyeball.
Course and prognosis • Depends on the severity of the primary injury - burns of I and II degrees have a favorable prognosis, complications often occur in degrees III and IV • For burns with acids, the prognosis is more favorable than for burns with alkalis • An increase in the area of perilimbal ischemia and corneal opacification indicates an unfavorable prognosis • Even with severe eye damage, permanent vision loss is not typical.
Age characteristics • Children. In children, eye burns are more severe due to the immaturity of the skin and eye structures • Elderly. In the presence of concomitant diseases (including dry keratitis), the prognosis is less favorable. Prevention . If there is potential eye contact with chemicals, safety glasses must be worn.
ICD-10 • T26 Thermal and chemical burns limited to the eye and its adnexa
Why is it necessary to go to the doctor after a chemical burn to the eyes?
Even if you feel better after first aid, ophthalmologists strongly recommend calling an ambulance or going to the hospital yourself. The fact is that sometimes the first symptoms may indicate a mild degree of damage, and after a day irreversible changes, such as blindness, may occur.
Doctors will help remove possible particles of foreign bodies and rinse the eyes again with neutral antiseptic solutions. They will also determine the severity and depth of the lesion and prescribe therapy based on this.
Ultraviolet eye burn: first aid rules
A burn of the cornea by ultraviolet light is called electroophthalmia. It often occurs in people who work with welding or are exposed to ultraviolet sun for a long time (for example, when skiing without a protective mask).
The peculiarity of an ultraviolet burn is that the first symptoms may appear only 6-10 hours after the injury.
First aid for ultraviolet eye burns is thorough rinsing with water or saline, instilling moisturizing drops and moving the victim to dark or low light conditions. You can also use sunglasses for this.
Anesthetics can be used briefly to relieve pain. But it is better to first consult with an emergency doctor, since such drugs slow down the healing process of the cornea. Cold compresses can help relieve pain without the use of medications.
To protect against infection, it is recommended to use antibacterial ophthalmic ointments.
An ultraviolet eye burn, if first aid is provided on time, is often a reversible condition and goes away without a trace within a few days. Moreover, electroophthalmia is easily prevented with preventive measures. For example, welders must use special protective masks when working, and skiers must wear ski goggles with high UV protection before skiing.
How to assess the degree of eye damage from a chemical burn?
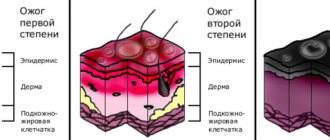
- I degree - superficial damage with slight redness of the eye shell (conjunctiva) and eyelids, a slight defect in the surface of the cornea. Does not require special treatment and does not threaten vision;
- Average, or II degree - superficial death of the mucous membrane of the eye and conjunctiva, swelling, damage to the transparent and epithelial layer of the cornea. Grayish-cloudy lesions on the surface of the eye, blisters and peeling on the skin of the eyelids may be visible. In such cases, scars may appear on the surface of the cornea and partial deterioration of vision;
- Severe, or III degree - damage to up to 50% of the surface of the eyeball. There is a process of tissue death throughout the conjunctiva and its lower layers, sclera and cartilage of the eyelids. If the eyelids are opened, the eye will look pale and very swollen. Due to a burn, the cornea loses its moisture and ceases to be transparent;
- Particularly severe, or grade IV - redness, swelling, darker areas are visible (deep necrosis). The conjunctiva and sclera darken. Due to a severe burn of the cornea, holes appear on it, it becomes gray, and the internal structures of the eye also suffer. At this stage, the likelihood of complete loss of vision is very high.
Characteristics and types of eye burns
According to statistics, approximately 10% of ophthalmic injuries are burns. At the same time, about 70% of victims receive burn injuries at work, and the remaining 30% - at home.
Essentially, an eye burn is damage to the cornea, eyeball, and other structures of the eye due to physical or chemical exposure. Depending on what caused the injury, there are several types of burns:
- chemical - when the damaging factor is aggressive chemicals;
- thermal - occurs when the eyes are exposed to hot air, liquid, steam, open fire;
- radiation - damage from ultraviolet, infrared rays or other types of radiation;
- combined - combines several damaging factors.
Taking into account the degree of eye damage, the burn can have 4 degrees. With the mildest, first, redness of the conjunctiva and skin of the eyelids occurs, swelling and superficial erosion of the cornea may develop.
In the second degree, the upper layers of the skin of the eyelids are damaged, burn blisters appear on it, and the epithelium and the underlying substance of the cornea are damaged.
A third degree burn injury is often indicated by severe clouding of the cornea - a burn in such a situation can even lead to the development of cataracts. Some of the tissues of the conjunctiva, sclera, and eyelid die, and the damage affects no more than half of the eyeball.
The most severe, fourth degree, is characterized by deep necrosis or charring of tissue. Often the patient develops uveitis, glaucoma, and perforation of the cornea.
There are also different types of burn injuries based on the location of the lesion: burns of the conjunctiva, cornea, eyelids, and periorbital zone.
Any burn to the eye area requires immediate first aid.
How are patients with chemical eye burns treated?
First, the hospital conducts diagnostics: they check vision, do an ultrasound of the organ of vision, biomicroscopy, measure intraocular pressure and perform a fundus check. This is necessary to assess the condition of the cornea, anterior chamber, lens, conjunctiva and eyelids. If the doctor detects signs of third or fourth degree damage, the patient is admitted to the hospital. In other cases, treatment at home, taking into account the recommendations of an ophthalmologist, will be sufficient. Typically, the ophthalmologist prescribes anti-inflammatory and antibacterial eye drops and gels for faster tissue healing.
Severe injuries may require surgery. It is done either in the first hours or days after a burn, if necessary to save the organ. Most often, surgical intervention waits until complete healing occurs.
Sources
- No authors found. // Zhonghua Yan Ke Za Zhi - 2022 - Vol57 - N4 - p.254-260; PMID:33832049
- No authors found. // Ophthalmologe - 2022 - Vol - NNULL - p.; PMID:33666702
- Claassen K., Rodil Dos Anjos D., Broding HC. Current status of emergency treatment of chemical eye burns in workplaces. // Int J Ophthalmol - 2022 - Vol14 - N2 - p.306-309; PMID:33614462
- Parmar DP., Bhole PK., Patel PN., Jadeja JN. Amniotic membrane transplant in acute ocular surface burns in Western India: A tertiary eye care center study. // Indian J Ophthalmol - 2022 - Vol69 - N1 - p.58-64; PMID:33323574
- Kulikov AN., Chernysh VF., Churashov SV. . // Vestn Oftalmol - 2020 - Vol136 - N2 - p.134-142; PMID:32366081
- Wiesner N., Dutescu RM., Uthoff D., Kottek A., Reim M., Schrage N. First aid therapy for corrosive chemical eye burns: results of a 30-year longitudinal study with two different decontamination concepts. // Graefes Arch Clin Exp Ophthalmol - 2022 - Vol257 - N8 - p.1795-1803; PMID:31147840
- Bizrah M., Yusuf A., Ahmad S. An update on chemical eye burns. // Eye (Lond) - 2022 - Vol33 - N9 - p.1362-1377; PMID:31086244
- Bizrah M., Yusuf A., Ahmad S. Adherence to Treatment and Follow-Up in Patients with Severe Chemical Eye Burns. // Ophthalmol Ther - 2022 - Vol8 - N2 - p.251-259; PMID:30868417
- Singh S.R., Yangzes S., Ram J. Saving the melting eye-alkali burns. // QJM - 2022 - Vol112 - N8 - p.621-622; PMID:30690637
- Arnljots T., Samolov B. . // Lakartidningen - 2022 - Vol115 - NNULL - p.; PMID:30277554
conclusions
Reference! Summarizing the above, it is worth noting:
- If acid gets into the eye, you must immediately provide assistance (or self-help) to the victim.
- If the situation does not improve within 24 hours, it is recommended to consult a specialist.
- To wash the acid, you can use a weak solution of baking soda, but do not use it on children.
- After providing first aid, the victim still needs therapy, which involves both conservative methods (eye drops) and surgical intervention.
Forecast
A chemical burn is a serious and emergency situation that requires immediate attention. Despite this, the prognosis in most cases is favorable. The main thing is not to panic and take all necessary measures.
Then doctors are able to completely preserve and restore the functions of the visual organs.
In industries with an increased risk of danger, workers undergo special training. Therefore, most people know what to do in an emergency. If there is no one near the victim, you must definitely call for help. The damage may cause blurred vision or an inability to open the eyelids. Therefore, the patient cannot help himself.
There are cases when timely, high-quality care cannot protect against the formation of a cataract on the injured eye. In addition, there is always a risk of atrophy of the eyeball, and subsequently loss of its mobility.
It is worth considering that preventing such damage is much easier than treating it. Complications can be very serious. Despite all the necessary auxiliary manipulations, you can lose your vision. It all depends on the substance that caused the burn and the extent of its damage.
When working with household products, it is important to prevent them from getting into your eyes. At enterprises, workers must be given protective uniforms and glasses. Especially those who come into contact with chemicals. Also, enterprises must have instructions for work and first aid rules.
If the employer does not provide the necessary protective equipment, this is considered a gross violation. Therefore, when working with chemicals and hazardous substances, this information must be taken into account. A person must be aware of the work rules and follow safety precautions.
Treatment
Immediately after an injury, cold compresses and lotions allowed .
You should know! Both regular ice or any frozen product may be suitable, as well as a lotion using herbal decoctions or infusions, which must be chilled.
In the evening of the same day, Cyclomed or Hydrocortisone ointment is applied . This should be done immediately before bed.
Then the doctor may prescribe eye drops , which need to be instilled 3-5 times a day, 1-2 drops.
These can be solutions of Balarpan, Levomycetin, Solcoseryl, Interferon , Albucid, Tsipromed, Oftan Dexomethasone.
Albucid 30% drops should not be instilled into a child without consulting a doctor.
For 2-3 days after the injury, you are allowed to rinse your eyes with a cool decoction of chamomile or calendula.
How to provide first aid at home
You should know! Providing first aid at home is not that difficult.
However, an adult and a child may need different help.
First aid for adults
The following actions must be taken:
- Remove any remaining irritant from the eyelids using a cotton swab or cotton swab.
- Rinse the eye generously under running water at room temperature (for at least 15 minutes). Next, it is recommended to wash the burn with a weak solution of baking soda (1 teaspoon or a little less per glass of water).
- Give the victim 2 painkiller tablets (Ibuprofen, Nise, Ketorol, No-shpa, Drotaverine, etc.).
- Drop a 4% solution of Novocaine or Lidocaine into the affected eye.
- After 20-30 minutes, drip 2-3 drops of any antibacterial agent (Levomycetin, Sulfacyl sodium). Or you can use Actipol - this drug relieves irritation of the mucous membrane.
It is worth noting! If the pain does not go away within 3-4 hours, you should consult an ophthalmologist.
First aid for a child
If acid gets into a child's eye, do the following:
- Remove any remaining irritant from the surface of the eyelids, eyelashes and skin around the eyes. This is necessary so that when washing the acid does not get on the mucous membrane again.
- Gently tilt the child's head and rinse the eye under running water at room temperature for 15 minutes.
- Give the child a painkiller tablet (you can use the same medications that are intended for adults).
- Give an antihistamine (Suprastin, Diazolin, Claritin, etc.). This will help reduce itching, irritation and swelling.
- Give the child eye drops to prevent infection (Levomycetin, Tobrex, Sulfacyl sodium, Actipol, etc.).
Important! It is not recommended to wash a child’s eyes with a soda solution or any other substances (potassium permanganate, tea, etc.).
After providing first aid, the baby should be shown to an ophthalmologist.
Features of burns with acids and alkalis
Eye burns from sulfuric acid are not as dangerous as from alkali. This is due to the fact that a film of coagulated protein forms on the eye when the irritant reacts with the mucous membrane. The film does not allow acid to penetrate deep into the eye, protecting the eye from deep damage. However, coagulation does not protect against complications if a concentrate of nitric and hydrofluoric acids gets into the eyes. An acid burn is characterized by severe pain, and sometimes even painful shock.
It is noteworthy that when the eye is damaged by alcohol, a person experiences severe pain, but minimal damage is noted. However, alcohol can absorb moisture from the lubricating fluid and the eyeball, penetrating deep into and damaging the cornea and lens. If washed in a timely manner, there will be no consequences for vision.
The most dangerous are alkali burns. In this case, there is severe dehydration and cell destruction. Alkalies provoke the decomposition of protein structures, wet necrosis develops, and when the irritant gets into the intraocular fluid, the deep structures of the eye are affected. Alkali can reach the corneal stroma and trabecular meshwork. As a result, the cornea becomes cloudy and intraocular pressure increases.
Common symptoms of a chemical burn
- Deterioration of vision. The initial decrease in visual acuity is caused by epithelial defects, increased lacrimation, clouding and discomfort. Even with moderate to severe burns, vision may be preserved if the corneal clouding is minor, but severe deterioration will occur over time.
- Fragments of the irritant in the arches of the outer shell. Residues of foreign matter are visible when plaster and other solid irritants enter the eye. The fragments must be removed immediately, otherwise they will continue to release toxins and worsen the damage. Only after cleansing the eye does the natural recovery process begin. Carbide and lime are the most dangerous because they dissolve in the tear and cause severe damage. If these substances come into contact, do not delay cleansing.
- Increased intraocular pressure. A sharp increase in pressure occurs due to deformation and contraction of collagen fibers in the anterior part of the eyeball. Subsequently, the increase is associated with inflammation.
- Inflammatory process in the conjunctiva. Even with mild damage, swelling and redness of the mucous membrane is noted. Sometimes when a burn occurs, the color of the conjunctiva changes (brown when damaged by chromic acid, yellowish when exposed to nitric acid).
- Perilimbal ischemia. Based on the degree of blanching, one can make a prediction about the restoration of the cornea, because limbal sprout cells restore the epithelium. Severe ischemia indicates an unfavorable course of the process.
- Cloudiness. If the cornea is transparent, a zero degree of damage is determined, and if the cornea is completely clouded, the fifth degree is determined. Complete stromal opacification makes it impossible to examine the anterior chamber of the eye.
- Defects of the corneal epithelium. Damage to the cornea can be expressed as diffuse punctate keratitis or complete absence of the epithelium. In the latter case, the defect is poorly stained with fluorescein and may not be diagnosed. If the epithelial defect is not visible during the initial examination, prompt re-examination is recommended.
- Corneal perforation. The symptom appears a few days after a severe eye burn, when the cornea's ability to regenerate decreases.
- Inflammation in the anterior region. The reaction may affect single cells or have a pronounced fibrinoid form. Inflammation is more pronounced when alkali gets into the eye, since these substances can penetrate deep into the structures.
- Scarring or other damage to the conjunctiva and eyelids. The symptom may be a problem if scarring prevents the palpebral fissure from closing.