1st degree burns are the most common type of domestic and industrial injuries. Surely many people during their lives have accidentally touched a hot object, a burning plant, such as nettle, been burned in the sun, or been scalded by boiling water. But even with a minor injury (to a hand or finger), you need to be able to provide qualified first aid for a 1st degree burn.
Minor burns can be successfully treated at home and do not require visiting a doctor. However, if the affected area is more than 10% of the total skin surface, you should immediately seek qualified medical help. To determine the degree of burn, you can check the table:
| Burn degree | Characteristic | First aid |
| I degree | Redness, swelling and tenderness of the skin | If the skin is not damaged, it is necessary to place the injured area under cold water for 10-15 minutes, then apply a sterile napkin. |
| II degree | The appearance of bubbles with liquid | If the skin is not damaged, it is necessary to place the injured area under cold water for 10-15 minutes, then apply a sterile napkin. |
| III degree | Dead skin, appearance of a scab (crust) | Cover the injured area with a clean, dry cloth and take to the doctor. |
| IV degree | Death of skin and tissue under the skin | Take painkillers and take them to the doctor. |
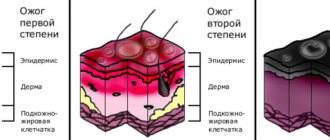
Classification of burns
Based on the depth of skin damage and includes 4 degrees.
- A 1st degree burn is the mildest injury and is characterized by redness of the skin.
- A 2nd degree burn is damage to the epidermis and underlying layer, characterized by detachment of the epidermis with the formation of “bubbles” filled with a clear yellowish liquid. The bottom of the burn surface is sharply painful. Bubbles can be of different sizes and shapes, often bursting on their own immediately after formation or when touching clothing or other objects.
- A 3rd degree burn is a deeper injury, in which, however, the germ layer of skin derivatives (sebaceous, sweat glands) is preserved. The blisters are filled with yellow, jelly-like discharge. The sensitivity of the wound bottom is preserved, but not increased. Due to the preservation of the germ layer, such burns heal quite quickly due to healing over the entire surface of the wound - from the preserved skin derivatives (sweat, sebaceous glands), the epidermis quickly forms over the entire wound surface.
- A 3rd B degree burn - with it, the germ layer is also damaged with the formation of blisters filled with brownish liquid or the formation of a brown scab. The bottom of the wound surface is completely devoid of sensitivity. Such burns heal much worse, because... Due to damage to the germ layer, healing does not occur over the entire surface of the wound, but only from the edges. With extensive (more than 50 sq. cm.) damage, skin grafting may be necessary.
- 4th degree burn – not only the entire thickness of the skin is damaged, but also the underlying tissue (photo below).
Burns 3B - 4th degree are deep. After such burns (especially extensive ones), rough scars can remain (photo below).
The area of the burn surface is of great importance.
Radiation burns (sun, welding)
Ultraviolet radiation (powerful light with an ultra-short wavelength invisible to the eye) primarily affects the skin of the eyelids, the conjunctiva and the cornea; the latter is the most dangerous. When damaged by light radiation in the infrared (thermal) range, the destructive flow reaches the retina and blood vessels.
These types of burns are usually associated with visiting solariums, unprotected presence in the area of electric welding or the action of a quartz lamp, as well as prolonged exposure to intense sun in blinding snow (especially in the polar regions). Symptoms usually develop several hours after the actual burn.
Radiation damage to the retina is a typical result of careless handling of laser equipment or unprotected contemplation of solar eclipses. In such cases, it may take several days for specific symptoms and/or decreased vision to develop.
The area is determined by several fairly simple and quick methods.
The "palm" rule - the surface of the victim's palm is approximately 1% of the surface of his body.
The rule of “nines” - the entire surface of the skin is conditionally divided into areas that are multiples of nine in area. Thus, the head and neck approximately make up 9% of the body area, the anterior surface of the torso - 18%, the posterior surface of the torso - 18%, the arm - 9%, the leg - 18%, the perineum - 1%.
There are also more accurate methods for determining area by measuring on graph paper with subsequent conversion to percentages, but they are not widely used and are used more for scientific purposes.
With burns of more than 15% of the body surface, burn disease develops - a severe violation of the general condition, accompanied by dehydration, shock, intoxication, the development of a septic condition, and failure of vital organs and systems. At the same time, burns of more than 40% of the body surface are considered very severe, and more than 80-90% of the body surface are often incompatible with life.
Contact lenses for burns
In 2013, Kemerovo scientists developed unique contact lenses that can significantly alleviate the plight of victims of eye burns. They are designed to provide pre-hospital medical care. Their use significantly reduces the risk of various complications.
The composition of these therapeutic contact lenses allows you to quickly neutralize hazardous substances that enter the eyes during a burn. They are simple and easy to use. The lens is easy to apply and remove and essentially acts as a sterile bandage to protect the injured eye.
These contact lenses allow you to speed up the process of eye recovery after a burn by 2-5 times. The speed of recovery will depend on the extent of damage to the eye.
Team of doctors Ochkov.Net
Treatment of burns
1st degree burns require virtually no treatment. In case of a 1st degree sunburn, you can wipe the reddened surfaces once with cologne or alcohol so that it does not get wet. If there are large areas, the victim must still be taken to a doctor; in some cases, bandages with chlorhexidine or miramistin are applied.
Treatment of 2nd and 3rd degree A burns includes excision of the exfoliated epidermis (blisters) and the use of therapeutic dressings with various agents (panthenol spray, etc.). It is a mistake to empty the blisters through a puncture, because... the remaining “skin” is still necrotic (dead), and wound discharge accumulates under it and microflora develops. In the normal course of the wound process, superficial burns heal in 7–14 days.
The photo below shows a 2nd degree burn in the ankle area.
The video below shows the treatment of this burn - the exfoliated epidermis is excised (anesthesia is not required, since the exfoliated epidermis is devoid of nerve endings), the wound is treated with an antiseptic and a bandage is applied with Panthenol spray.
The photo shows a 3A degree burn, with 3B degree elements in the center. Good epithelization is visible from the edges where there is a 3A degree burn. In the center, where there was a 3B degree burn, the wound is clean and granular. Such a burn will heal quickly, but not immediately over the entire surface, but gradually, from the periphery to the center.
Burns of the 3rd B, 4th degree take much longer to heal due to the necrosis of the germ layer of the skin. Along with dressings, they often require excision of dead tissue (necrectomy), and for large surfaces - skin grafting (skin grafting).
First aid
Of course, the first and most urgent measure is to remove the eye from the influence of the damaging factor and deliver the victim to the nearest specialized medical facility as soon as possible.
At the same time, in most cases (EXCEPT FOR LIME BURNS!) you can rinse the eye with clean water and drip any antibacterial drops (Albucid, Levomycetin, etc.). It will be useful to apply a bandage (not pressing) to reduce the movement of the victim's eyes.
Chemical burns
The manifestations are similar to thermal ones, but due to the aggressiveness of the damaging agent, severe forms of burns predominate: 3rd B, 4th. The toxic effect of the damaging substances themselves (acids, alkalis, etc.) on the body as a whole is also added due to their absorption from burn surfaces. As first aid, a long period of 10-15 minutes of rinsing the damaged area with a stream of water is necessary.
The photo shows a 3B degree chemical burn on the foot. The patient made a compress of vinegar to self-treat foot fungus. On the foot and toes there are superficial necrosis (scabs) of brown color.
The photo below shows the same burn 10 days later during treatment - the scabs have come off, the wound surfaces have cleaned and are healing.
Symptoms
Depending on the specific damaging factor, the clinical picture of an ophthalmic burn may vary, but the most typical symptoms are:
- redness and swelling of the eyelids;
- swelling of the mucous membranes (conjunctiva of the inner surface of the eyelids and eyeball);
- general redness of the eye;
- intense, even unbearable, pain;
- blepharospasm (involuntary contraction of the muscles that control the movement of the eyelids);
- painful reaction to light, even soft and diffused;
- increased lacrimation;
- inflammation of the blood vessels of the eyeball;
- abnormal values of intraocular pressure (both hypo- and hypertension are possible);
— clouding of the cornea;
- a sharp deterioration in visual acuity and clarity, narrowing of the fields.
In case of radiation injury, symptoms may initially be limited to the latter symptom; with an infrared or laser burn, the affected tissue intensively scars, and vascular neoplasms appear (neovascularization).
There are four degrees of burn severity. Of course, the specific degree of damage depends on many factors (physical and/or chemical characteristics, total area of damage, duration of destructive effects, etc.).
Starting with a second degree burn, hospitalization is mandatory.
THE SKIN WILL NOT BE THE SAME AS IT WAS BEFORE THE BURN – WHAT ELSE IS IMPORTANT FOR PATIENTS TO KNOW
How are patients with burns treated today, why can’t this be done without psychologists, what does a doctor do when a teenager doesn’t want to go to prom because of scars on his neck, and will we stop paying attention to unusual skin? Doctor of Medical Sciences, Professor, Head of the Burn Center at Children's Hospital No. 9 named after A. G.N. Speransky Lyudmila Iasonovna Budkevich
A mug of tea on the table, an iron placed on the floor, a hot grill - most burns in children occur due to the carelessness of adults. Forty years ago, pediatric surgeon Lyudmila Budkevich came to work in the burn department and in the first six months wrote a letter of resignation three times, but always stayed. She is known as the head of the burn center of Moscow Hospital No. 9 named after G. Speransky, where children from all over Russia are treated.
– How is it that almost three thousand children come to you every year with burn injuries?
– For some reason, our parents think that trouble can happen to someone else, but not to their child, and most often children under 3 years old get burns at home, due to some kind of carelessness of adults. Just today we discharged a boy who fell face down on a hot grill and received a burn to his face and a cut wound to his lip! Our children are burned by hot liquid - the child curiously reaches for a cup of coffee, throws hot milk or soup over himself, comes into contact with a heated surface - he puts his palm against the burner that is on, against the oven door, against the iron that has just been turned off and for some reason placed on the floor . A child can take any metal object and insert it into an outlet that does not have a plug, or grab a bare wire from a non-functioning household appliance, such as a TV or radio.
– Is there any concern that the house could be so dangerous?
- Exactly! And a small child in the first years of life can get a deep burn, when the skin is damaged to the full depth and sometimes even the underlying tissues, by pouring a glass of water over 45 degrees on himself. Burns up to 30% of the body surface, and irreversible consequences for the skin. Chemical burns occur: for example, a child drinks or spills surface cleaning liquid left open on himself. And it contains alkali, which causes damage to the skin and mucous membrane of the gastrointestinal tract. We notice that burn injuries have a certain seasonality: in winter they are caused by hot liquid, and in summer they are caused by flames. Contrary to instructions, adults pour fire starter fluid onto smoldering coals or firewood, causing an explosion and igniting clothing! There have been cases where a child stands with his feet on hot coals. Summer is characterized by “hookers” - teenagers who run on the roofs of electric trains, getting pleasure and some kind of courage from it, touch the wires, lose consciousness and fall on the platforms, breaking their arms and legs. You see, it only takes a second for a child to get injured, and believe me, in this short time, life is instantly divided into two periods “before” and “after”, problems appear that change the entire subsequent life of not only the child himself, but also his family.
– But if an injury does occur, what would you recommend doing or not doing?
– As a rule, no matter what the thermal burn, with the exception of electrical trauma, you need to pour water over the area at a temperature of 25-27 degrees and keep it there for five to seven minutes to cool the wound surface. This is the very first event that is necessary. At the same time, if clothing catches fire, you should not tear it off the child - thereby we injure the damaged skin. It is necessary to put out the fire and call an ambulance so that, if necessary, the child is hospitalized in a specialized hospital. And the doctors will already figure out what to do next. I do not recommend self-medication. There are a lot of folk remedies, but most often they are harmful. For some reason, grandmothers recommend using sunflower oil, but it only creates a film on the wound surface and prevents the evaporation of heat from the tissue into the environment, and this deepens the burn. For some reason, they use honey or potato cakes, which themselves can cause a burn - mom in a hurry will not feel the temperature of the potatoes. Toothpaste, especially mint, does have a cooling effect, but again you have to wash it off, which is painful. And aerosols with an orange color prevent us from determining the depth of the damage.
Ashina disaster: there were no children with burns of less than 50% area
– Is it true that forty years ago doctors did not want to work in burn departments and often ended up there for some kind of misconduct?
– You know, I found a period in the early 1980s when few surgeons voluntarily went to work in the burn department. Patients are the most difficult and unpredictable in terms of disease outcome of all surgical patients. The treatment used outdated methods known since the Second World War. As a rule, the so-called chemical necrectomy was used to remove necrotic tissue, in which the wounds were cleaned no earlier than the 3rd week of the disease. There was no adequate pain relief. I found myself in such a department, as a sixth-year medical student, I will never forget this smell... And not everyone can withstand the moans and screams of adult patients, not to mention children, so it’s true that most often doctors ended up with burns for some kind of misconduct in of their professional activities. During the first six months of work at the burn center of the children's city hospital No. 9 named after. I wrote a letter of resignation to G.N. Speransky three times, believe me. And although by that time I already had ten years of experience as a pediatric surgeon, for some reason I could not calmly see these suffering children. At that time, there were many children with amputated limbs, with severe burn injuries caused by flames and electric current. And I was a young mother, and I blamed this misfortune on my sons. But life developed in such a way that I stayed for one reason or another.
– Why did you even start working in the burn department?
- That’s how it turned out. People often become combustiologists by pure chance (smiles). I wanted to do science and be an ultrasound diagnostics doctor, but there were free positions for research assistants only in the department of thermal injuries at the Research Institute of Pediatrics and Pediatric Surgery. I thought I’d work here temporarily, and two months later the head of the department asks me: “What topic will you write your dissertation on?” And so I became a combustiologist.
– What topic did you choose for your dissertation then?
– My dissertation research was called “Criteria for the readiness of a burn wound for skin grafting.” In 1988 I defended myself and was offered the position of head of the newly opened burn department for young children (the first three years of life). It must be said that such a department is the only one not only in Russia, but also in the world. Just that year, a law was passed that women could take leave to care for children up to 3 years old, and, oddly enough, the number of children with burn injuries increased. And a year later, in 1989, there was a railway accident near Asha (the largest in the history of the USSR and modern Russia. At the moment of the meeting of two passenger trains No. 211 “Novosibirsk - Adler” and No. 212 “Adler - Novosibirsk” due to a gas leak from a gas cloud exploded on the main product pipeline, killing about seven hundred people - ed.), and I and another surgeon from our clinic were delegated to help our colleagues, doctors at children's hospitals in Ufa, where the burned victims were admitted. There were no children with burns of less than 50% area. But the most deplorable impression was made by the trip to the scene of the disaster. The territory within a radius of 500 meters was completely scorched, covered with ashes, children’s shoes and toys were lying under it... In those days, one journalist asked me: “How do you relieve stress?”, and I answered: “The smile of a recovering child is the best medicine,” and for me it still is. Of course, psychologists worked with us, but then there was no time to think about ourselves - there were many sick people, there were cases of death. We took the 28 heaviest children by air to our burn center in Moscow. This tragedy marked the beginning of the creation of the All-Russian Center for Disaster Medicine “Zashchita” and the Ministry of Emergency Situations.
– After the Ashin tragedy, did your attitude towards the profession change?
- Undoubtedly! Since then, I have not imagined myself in another branch of medicine. Soon we began working with combustiologists from England and the USA (project “Nadezhda”). The British founded the Friends of Russian Children foundation. The doctors of our burn center and I went abroad for internships, where we became acquainted with modern methods of diagnosing burn injury and its complications, and mastered innovative surgical interventions for victims with deep skin burns. And, of course, thanks to new technologies in all areas - anesthesiology service, antibacterial therapy, and surgical treatment - we began to care for even the most seemingly hopeless patients, who were doomed in the 70-80s.
Treatment of a deep burn is not just a “patch” on the skin
– What does the process of treating children with burns consist of?
– When the wound area is 10% of the body surface or more, children experience burn shock - a process in which not only damage to the skin occurs, but also functional disorders in the victim’s body. And it is urgent to get patients out of this state. Sometimes medical assistance is needed during the evacuation stage.
We had such a case: trouble happened on the river bank, teenagers were riding a motorcycle and a gasoline tank exploded, the guys received deep burns covering an area of 45-50% of the body surface. The burn center is more than an hour and a half away, so it is necessary to carry out resuscitation measures already in an ambulance - place a peripheral catheter in a vein to carry out infusion therapy. It all depends on the severity of the condition. And then the surgeon determines the area of the burn wounds and the depth of the lesion. There is a slightly primitive, but easily accessible “rule of the palm”, that is, each patient’s palm is equal to 1% of the body surface. And to imagine the area of the wounds, you can visually project the victim’s palm onto the wound surface, for example, 30% is thirty child’s palms. This method is good for emergency doctors and nurses. We use formulas for accurate calculations - the volume of infusion therapy depends on it. Next, the doctor performs primary surgical treatment of the wound - treats the surface with an antiseptic solution, and then opens the epidermal blisters. If they are not opened in time, the contents of the blisters from the surface of intact skin will become infected. But again, I don’t recommend doing this yourself. And only then they apply atraumatic mesh coverings to the wound surface. Such meshes do not stick to the wound, making it easier to change dressings. And then, for three days, we observe the picture of changes in the surface of the wound and decide how the skin will be restored: local conservative therapy (independent epithelization of wounds) or surgical treatment (removal of necrotic tissue with skin grafting of the wound defect).
– How is the operation going?
– First, necrotic dead tissue is removed, bleeding is restored, and then a skin graft is taken from the donor site, that is, a piece of healthy skin 0.1-0.2 mm thick, and transferred to the wound. This is a kind of “patch”. If we have a shortage of donor areas of healthy skin, for example, when the burn area is 30-40% of the body surface, and we need to grow cells, then we use foreign skin, xenoskin, taken from animals, in particular from pigs, as a temporary biological covering. And thereby we protect the wound from external mechanical influence and infections, and prevent the loss of fluid and microelements from the body. And after the donor sites are ready to take the split skin graft again, we remove the pig skin - it played its role - and transplant the newly taken skin. But treating a patient is a team effort. This is not only a combustiologist involved in wound management. We need to overcome the period of acute burn injury while maintaining the functions of vital organs. Professionally trained resuscitators and pediatricians help us with this.
Patients may have problems with the gastrointestinal tract - they need a gastroenterologist and nutritionist (medical nutrition doctor). In children of the first three years of life, the central nervous system always suffers due to its underdevelopment - we cannot do this without consulting a neurologist. If the eyelids are damaged, be sure to see an ophthalmologist to rule out eye injury. When the cartilage of the nose or ears burns, an obligatory examination by an otolaryngologist is necessary. Sometimes burn injuries are combined with mechanical ones. The same “hooks”, touching the wires with their heads or hands, lose consciousness from the effects of high voltage current, fall onto platforms, break the bones of their arms and legs, and cases of traumatic brain injury are not uncommon. And here we need traumatologists and neurosurgeons. And when the burn wound is located circularly on the limbs, we invite our fellow traumatologists to install external fixation devices that facilitate wound care. Without an anesthesiologist, we cannot carry out dressings and surgical interventions to close burn wounds. A hematologist is responsible for blood transfusions, clinical pharmacologists are responsible for antibacterial therapy, laboratory assistants are responsible for the accuracy of tests, and rehabilitation specialists are responsible for preventing the formation of severe scars in patients with deep burns. Psychologists - for the emotional state of patients, art therapists - for socialization after recovery and return home. This is truly a team method of treatment; without such a number of medical workers, we cannot make the patient healthier.
– What scientific discoveries are you looking forward to?
– We hope that they will soon print leather on a 3D printer. And such work is already underway. Cell laboratories will be organized in which skin cells are grown, so necessary for our patients with a severe shortage of donor sites in case of extensive burns.
– In your opinion, will it ever be possible not to be afraid of burns?
- Unfortunately no. The course of a burn injury is influenced by various factors - diseases that existed before the injury, age - infants and old people suffer more severely, the area and location of the burn, the state of immunity of the burned. There is a medical term “injury incompatible with life,” and there are cases when doctors are unable to help patients. Sometimes extensive burns of the skin over 50% of the body surface are combined with a burn of the respiratory tract mucosa (thermal inhalation injury). In such a situation, the total area of burn wounds increases by another 15% of the body surface. The patient has been on artificial ventilation for a long time. And, as a rule, severe complications arise in the form of purulent tracheobronchitis or pneumonia. It is difficult to fight a purulent infection when all the patient’s organs and systems are involved in the inflammatory process. Symptoms of central nervous system dysfunction appear in the form of burn encephalopathy, which is manifested by the victim’s excited state, hallucinations, monotonous crying or screaming, sometimes convulsive readiness in the form of tremors of the limbs, turning into convulsions, which requires analgesic, anticonvulsant, sedative therapy against the background of artificial ventilation. At the same time, the liver suffers (toxic hepatitis), the heart suffers from myocarditis, and the kidneys suffer from acute renal failure. Against this background, stress ulcers of the gastrointestinal tract occur (due to oxygen starvation of the tissues of the mucous membrane of the stomach and duodenum); in some cases, bleeding from the vessels of the resulting ulcers is diagnosed. Patients may die from intractable gastric bleeding. In patients with extensive skin burns and, as a consequence, dysfunction of body organs, generalization of infection occurs with the development of sepsis, which is the main cause of death in burn patients. But still, as I already said, we have now learned to care for completely hopeless patients.
Once a boy from Magadan was rescued with a burn on 95% of the surface of his body; he received burns in a house fire. The boy was evacuated to our clinic, since specialized medical care for patients with extensive burns is not always available locally. But these children and their parents have many problems.
No need to constantly look at these scars!
– What are these problems? Aesthetics are understandable...
– I always say that burn injury is a social problem. Unfortunately, deep burns heal by forming a scar, which, yes, can form in aesthetically important areas - on the face, in the collar area, neck, anterior chest, hands and feet, as well as in the area of large joints - and this causes contractures , tightening of the skin, due to which children cannot fully straighten or bend one or another joint. If the injury is on the hand, then the fingers function poorly, and often a large number of corrective surgical interventions are required to straighten these fingers and make them functionally active. If contractures interfere with the development of the skeleton, it is necessary to operate again, otherwise the child will no longer care for himself. Children who have been diagnosed with a disability must have it confirmed annually. And to avoid a relapse, you need to constantly do massages, wear special compression clothing, mud and paraffin therapy is necessary. It happens that deep burns end in amputation, so prosthetics are necessary for such patients. The child grows and the prosthesis needs to be replaced multiple times. And even after surgical interventions, the skin will not be the same as before the burn injury...
– If a child in your center asks for a mirror, with what words do you give it?
– You know, we don’t have mirrors in the burn center - it just happened that way, and as a rule, children don’t ask for mirrors, and if they do, it’s certainly not from doctors. Here they are emotionally stable, because they see boys and girls just like them, and when they find themselves at home alone with trouble, then emotional breakdowns begin.
Psychologists and art therapists have been working at our advisory clinic for many years. They work not only with children who have suffered burn injury, but also with their parents. Patients who have suffered thermal injury are under the supervision of clinic staff until they are 18 years old. These specialists help former patients find their place in life.
Our charitable foundation "Children's Hospital" organizes winter and summer camps for those who have suffered severe burn injury - children go to boarding houses in the Tver and Yaroslavl regions. After spending time together in nature, children and their parents communicate with each other, correspond, and consult with each other on what to do in certain health-related situations. All this has a beneficial effect on the quality of life of our patients.
– What words do you use to discharge children and parents?
– There is no stencil, it all depends on the situation (smiles). We recently treated a young man with a large area of wounds, and he was from a cadet school. And I told him: “You will be an officer! Everything works for you - arms, legs, and you can’t see the scars under your jacket.” And naturally, we also work with parents.
– What is important for them to understand and know?
“I always tell the relatives of our patients not to make their children disabled. “You don’t have to constantly look at these scars, because the child feels like his mother is looking at him! Your child is normal, healthy, he just has different skin. After all, there are people with yellow or black skin.” You see, these children should grow up normal, just like before the injury, and play sports - there are no contraindications to this. Well, let the child wear compression clothing - this is not a hindrance, it is the same clothing that can be taken off and put on again. We always work positively, do not let parents and children become discouraged, and find kind words in any situation. If adults, after discharge from the hospital, do not perceive the child as they did before the injury, then the problems will grow like a snowball. It is parents who become the main teachers in life and show children how to behave and instill confidence in their own abilities. I think we need to develop in a direction where there are social workers who, even before the child returns from the hospital to his usual environment, visit kindergartens or schools where this or that patient will return, and conduct explanatory conversations with the children, teachers and educators about how to behave correctly with children who have suffered burns.
– Can a doctor tell parents that the child’s burn was their fault?
- No, the doctor does not tell mom or dad that they are to blame for what happened. But, unfortunately, not every parent understands this themselves; some come with the words “And this is the second time we’ve visited you!” Sometimes mothers withdraw into themselves, and then we schedule a consultation with a psychologist. If adults do not pull themselves together, thereby not emotionally participating in the treatment process, then it is not always possible to quickly achieve the desired results. I always tell my employees that they need to sympathize with parents and take their place. We treat our patients like our own children, and my sons, when they were younger, repeatedly said: “You love your patients more than us.”
– Did you change anything in the arrangement of your home when you started working with burns? Maybe they also became more attentive?
– I don’t want to praise myself, but... I live by the rules and ask those around me to follow them. Place the pots on the last row of burners. Before putting your baby in the bath, you should test the water with your elbow, where the skin is most sensitive. Children should not be in the kitchen while food is being prepared. You need to iron when the child is sleeping, and remember that the floor is not a place for a hot iron. Anything dangerous must be removed. Electrical sockets must have plugs. Well, I don’t know... I was raised this way and I hope that my sons, one of whom already has their own children, remembered these rules. But even now I often remind them of the dangers that exist in the house.
The most harmful thing is bad manners
– What would you say to a stranger who looks askance at a person with a burn?
“You, too, can end up in this place at any time; no one can guarantee you that you will be a healthy person forever.” After all, a burn patient is exactly the same person, he just has unusual skin. Why turn around and discuss in the back? I think that the most destructive quality in people is bad manners in any of its manifestations. And why doesn’t our employer hire a salesperson with hands that have scars on them? This is exactly the same skin, it is washed with soap in the same way, it is not contagious! But why? You know, I keep in touch with many former patients. Many of them have higher education, are married, and have children. Recently, a former patient Valechka came to our clinic for an open day; she had a burn on her face and scalp, which she received as a newborn child. And now she already has her own child!
And the other day I received a call from the mother of a patient who was about 2 years old when he was hospitalized with us for a burn. Now he is 24 years old, he has become a doctor, he wants to join us as an anesthesiologist, so that he can also help sick children.
– But do those who have extensive burns experience gratitude and joy?
“We immediately warn parents and older children not to expect that they will develop the same skin as before the injury. Teenagers are often capricious, and they have to explain that if this procedure is not done now, they will have certain health problems that will be difficult to solve later. Treatment of a burn injury involves constant monitoring to ensure that complications do not occur. And our job is to treat patients and strive to ensure that the consequences of a burn for them are minimal.
– Has your attitude towards appearance changed in any way over almost forty years of working at the burn center?
– You know, I am very critical of my appearance and always say that “don’t drink water off your face,” and appearance doesn’t matter at all. You communicate with a person, and not with his appearance, and, probably, you are interested in his character, attitude towards others, and not what shape his nose is and whether his eyelids are his own or artificially made. Wisdom comes with age... As a rule, people become wiser after thirty. I think wisdom in terms of attitude towards appearance also comes to our patients. Of course, it’s nice to look at a beautiful person, but you definitely shouldn’t judge him by his appearance.
“Can you tell that to a teenager?”
- Certainly can! Why not say if he’s already big and understands everything? I have a patient - he is now 25 years old. At the age of 3, he received a severe burn injury and was in extremely serious condition for a long time. We managed to save him. But rough post-burn scars formed on the neck and face. How complex he was! He wore turtlenecks all the time or tied a scarf around his neck, regardless of the time of year, to hide the consequences of the injury. The school graduation ceremony has arrived. His mom (she's pure gold!) bought him a suit. And I - a shirt with a turn-down collar that would cover the scars on my neck. I say: “Sasha, on this day you should be the most elegant and beautiful!” And he forced himself to put on this shirt. Over time, the boy grew up, and his opinion about his appearance changed. He is married and works as a successful lawyer. Life is good! Believe me, I can find so many positive qualities in a person, so much positivity that can overshadow all his complexes! It is necessary to draw the child’s attention in time to that “zest” in his character, which will become important and life-affirming for him.
– Is this also a doctor’s task?
- A doctor is also a person. Sometimes I really want to compliment a stranger on the street. And sometimes I restrain myself, and sometimes I speak. Why not say if a person, for example, has a very beautiful dress or hat? We say so few kind words to each other!
- And how do they react?
– They smile more often. Maybe they think: “Crazy” (laughs). And you know, sometimes I see a person with burns, and I just want to come up and advise where they can help correct the scars. If I know, why not tell me? But again they will say that... But since I recently started praising those around me, maybe I’ll start giving advice.