A thermal burn is a specific injury to the skin and (sometimes) underlying tissue due to exposure to high temperatures. Sources of thermal effects can be both solids and liquids, as well as steam or gas. As a rule, contact with a carrier of excess heat occurs as a result of a violation of safety standards for working with its sources or as a result of an accident. Sunburns should also be partially classified as thermal. They arise due to the combined effect on the skin and mucous membranes of both ultraviolet rays, which themselves have a destructive effect on the body, and the thermal energy of solar radiation.
When exposed to thermal energy, the body primarily injures the skin (or mucous membranes). If the intensity of the thermal effect is high, then the injury can affect not only all layers of the skin, but also the tissues located underneath it. Depending on the depth of tissue damage, in clinical practice there are 4 degrees of burns, each of which has its own symptoms and clinical features, on the basis of which the treatment program is based. Therefore, before moving on to considering the treatment of thermal burns, you should familiarize yourself with them.
LEATHER. SKIN STRUCTURE. SKIN FUNCTION
SKIN is one of the most complex organs of our body, subject to the strongest physical and physiological stress. Skin is the largest organ of our body. The complex structure of the skin with its numerous vessels, nerves, sebaceous and sweat glands is necessary to perform certain functions.
Skin is: -Preventing fluid loss by the body; -Protection of internal organs from the negative influence of external influences; -Ability to evaluate pressure, touch and vibration. Nerve endings and receptors inform the body about temperature and pain effects; -Barrier functions. This is protection against bacteria and microorganisms; -Protection from ultraviolet radiation; -Maintaining optimal body temperature.
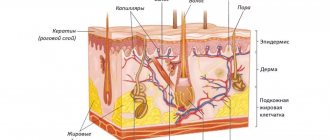
The skin consists of two layers: EPIDERMIS and DERMI
. Under these layers is subcutaneous fatty tissue.
EPIDERMIS
- avascular upper thin layer of skin (does not have its own blood supply). The epidermis receives nutrition from the capillary bed of the dermis due to the diffusion of nutrients. The epidermis consists of numerous layers of living cells, on top of which are dead cells.
The layers of the Epidermis can be represented as follows:
- Basal (germ layer).
The lower layer of the Epidermis. Consists of cells capable of regeneration (cell division) - cylindrical keratinocytes. The basal layer ensures constant regeneration of the Epidermis, however, cell division is regulated by certain factors: hormones, vitamins, kelons. Keylons are simple substances that suppress growth and regulate the functioning of the basal layer. Thanks to keylons, basal cells have limited growth (proliferation). Beneath the stratum basale is the basement membrane, which separates the stratum basale from the dermis. - Spiny.
Contains up to 6 layers of irregularly shaped cells. They have little activity for cell division (limited mitotic activity). - Grainy.
The death of Epidermal cells begins in this layer. Contains up to 3 layers of cells. - Brilliant.
The stratum pellucida consists of anucleated cells in which intense enzymatic activity is observed. Eleidine is formed in the stratum lucidum. Eleidin is a substance rich in fats and proteins with a high refractive index of light, looks like a homogeneous dense shiny layer, which gives its name to this layer of cells. The shiny layer protects the body from the effects of various aqueous solutions. - Horny.
The stratum corneum consists of anucleated keratinized cells (keratin is a protein that has high mechanical strength and performs protective functions), which are called corneocytes. The cells of the stratum corneum lie with some overlap, like brickwork, and are firmly connected to each other by the finest fibers (tonofibrils). The stratum corneum has 15 to 20 layers of cells, with the outer layer continually being shed as detached flakes of skin.
So, in general, the Epidermis works like this: in the lower, basal layer, cells are constantly dividing. After division, one of the newly formed cells passes into the next layers of the Epidermis. From layer to layer, cells lose contact with nutrients coming from the Dermis and lose the ability to divide. The closer a cell approaches the surface of the skin, the more strongly external environmental factors begin to act on it, keratinization of the cell occurs, the cell loses its nucleus and turns into a scale of the stratum corneum.
The stratum corneum, the upper layer of the epidermis, easily allows low-molecular substances such as oxygen from the environment to pass through. Bacteria, which are significantly larger in size, are not able to overcome the upper layer of the Epidermis, therefore the Epidermis is the skin protection that is optimal for the body. In the Epidermis, the processes of cell division of the lower Basal layer, regulated by keylons, the gradual transition of cells to the upper layers, transformation into keratin scales and, finally, exfoliation of the outer scales in the stratum corneum occur in a balanced manner. Complete renewal of the Epidermis lasts from 10 to 30 days.
The high strength of the Epidermis serves as a good barrier to various substances and does not allow them to penetrate the body. This also applies to most cosmetics.
DERMIS
- the frame, the skin itself, which provides its mechanical properties: elasticity, strength and extensibility. These properties are provided by connective tissue that has elastic fibers, Elastin, which allows the Dermis to stretch, and collagen fibers, which strengthen the Dermis.
The following structures are located in the Dermis: blood vessels, sweat glands, nerve endings, hair roots with sebaceous glands. Deeper is the subcutaneous fatty tissue - the hypodermis. It absorbs the effect of mechanical factors on the skin and participates in the thermoregulation of the skin. In this part of the skin there are clusters of fat cells separated by bundles of collagen fibers.
KEYLONS. A LITTLE ABOUT THE MECHANISM OF CELL CYCLE REGULATION
Research in the field of skin regeneration and the general mechanisms of the cell cycle has been conducted since the middle of the last century. R. Weiss and J. Kavanau, W. S. Bullough and T. Rytomaa, V. I. Prilutsky and Yu. A. Romanov are the founders of the theory of cell division. P. Nurse, Leland H. Harwell and R. Timothy Hunt are modern researchers of the principles of regulation of the work of individual cells and the body as a whole.
Disruption of the process of cell division (impairment of cell mitosis) is a source of not only cancer. Limited regeneration leads to aging of cells and aging of the body as a whole. In case of injuries and pathologies, low tissue regeneration significantly prolongs the healing process.
Outstanding examples of self-repair are known to everyone: severed tails, damaged hearts, and spinal cords in amphibians are restored (repaired) in a very short time. What signals does the body give to tissues so that they begin to grow, what is the growth factor? But first, about the life path of cells. A cell is the elementary unit of all living organisms. All living things are made up of cells. Regeneration, cell reproduction by mitosis occurs as follows: genetic material is reproduced inside the cell (this ensures the genetic identity of the daughter cells), after which the cell divides.
The process of cell division from the start of the mechanism to the actual division is called proliferation. Proliferation is regulated both by the cell itself and its environment. The main signal for triggering the cell division mechanism is provided by the plasma membrane of the cell. The membrane has special receptors on its surface that evaluate the “environment” around the cell and trigger the process of proliferation. These signals can come from neighboring cells, as well as from the interaction of cells with various compounds that stimulate entry into the cell cycle. These compounds are called growth factors.
But in tissues there are also substances that limit cell division. These are the Kaylons.
Keylons
- substances contained in tissue (simple proteins or glycoproteins) that specifically suppress cell division and DNA synthesis in this tissue. Keylons do not have species specificity. The action of kelons is to suppress or slow down the rate of cell division in the tissues that produce them. For example, keylons of the Basal Layer of the Epidermis act only on the Epidermis.
Cell regeneration is described by a growth regulation model. This model explains how body tissues carry out self-regulation. Any tissue capable of regeneration consists of two types of cells: cells capable of dividing and cells that cannot divide: proliferating and differentiated cells. The behavior of proliferating cells is controlled by differentiated cells: Kaylons are produced in differentiated cells and act on cells capable of dividing - proliferating cells. If for some reason the number of differentiated functioning cells decreases (for example, after injury), the inhibitory effect of the keylons weakens and the population size is restored. This ensures a balance between tissue growth and loss and explains the regeneration process.
WOUNDS. BURNS (BURN WOUNDS). TYPES OF BURNS
A wound is any open injury associated with a violation of the integrity of the skin or mucous membranes, with possible destruction of underlying tissues.
Wound healing is the wound process of restoring damaged tissue: restoring its integrity and strength.
Depending on the nature of the damaging factor, wounds can be divided into the following types: Mechanical, Burn, Chronic (trophic skin ulcers). In the presence of several types of damaging factors, the wound is usually called combined.
Wounds are dangerous
primarily bleeding, and, as a result, the development of anemia. As a result of the shock received from injury, dysfunction of vital organs can occur. Depending on the cause of the injury (the etiology of the wound) and the size of the wound, the body may become infected.
The problem of intoxication of the body is especially acute with large areas of burn wounds.
BURN - damage to tissue (skin or mucous membranes) under the influence of various factors: high temperature (thermal burns), chemicals (chemical burns), ultraviolet or ionizing radiation (radiation burn), electric current (electrical burn).
BURN. GRADES OF BURN WOUNDS
The severity of injury in a thermal burn is determined primarily by the depth and area of the thermal injury:
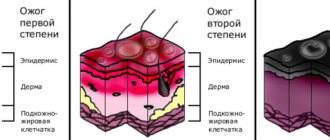
First degree burn (epidermal burn): redness (hyperemia) and slight swelling. Only the Epidermis is affected. Treatment under bandages or open method. Hospitalization is indicated for burns of more than 15% of the body surface.
Second degree burn (superficial dermal burn): the appearance of “bubbles” filled with serous contents. Peeling of the epidermis. The epidermis and upper layer of the dermis are affected. Outpatient treatment is allowed if the burn area is less than 10% and anatomically significant areas (face, neck, perineum) are not affected. But hospitalization is possible depending on the area of the burn, its location, and the age of the patient.
IIIA degree burn: Skin after a burn is diagnosed by a thin mobile scab and large blisters filled with serous contents with an intense yellow coloring. The Epidermis and Dermis up to the reticular layer are affected. But the follicles, sweat glands, and omental bursae remain undamaged by the burn, which will initiate epithelization of the wound. IIIA degree burns are called borderline, because... the lesion is not uniform over the entire surface. The burn can go deeper into the underlying tissues, including due to infection. Victims diagnosed with a IIIA degree burn can be treated on an outpatient basis if the burn surface does not exceed 5% of the body area and no significant anatomical areas are affected.
IIIB degree burn: The entire thickness of the skin is affected: up to the subcutaneous fat. A brown scab forms on the surface. Requires surgical treatment.
IV degree burn: The skin is affected to its full depth and the underlying tissue is destroyed. Subcutaneous fat, muscles and bones are charred. Diagnosed by a dense dark brown or black scab, fused to the underlying tissues. Requires surgical treatment.
Burns. Pathogenesis classification.
BURN (combustio) is a specific damage to tissues and organs caused by exposure to thermal, chemical, electrical or radiation energy.
Etiology. According to their physical nature, thermal agents can be divided into solid, liquid and gaseous. Based on the type of interaction with the victim’s tissues, contact lesions are distinguished (with direct interaction with the victim’s tissues: flame, hot liquids, etc.) and distant (without direct contact: ultraviolet, infrared, thermal radiation) lesions.
Pathogenesis of local changes in skin burns.
The optimum temperature for the activity of many biologically important enzymes corresponds to 36-37˚С; the temperature range from 37 to 41˚С for the skin is acceptable; further heating leads to cell damage. The duration of tissue hyperthermia many times exceeds the duration of action of the thermal agent itself.
When exposed to high temperatures, burns of various degrees are formed on the surface of the body. When tissues are overheated above 520C, coagulation coagulation of proteins is irreversible. The consequences of burns depend on the size and depth of tissue damage.
There are 3 concentric zones of damage for deep burns, depending on the degree of circulatory impairment. The central area of the wound, which is most closely in contact with the heat source, is called the coagulation zone. Around it there is a zone of paranecrosis, called by Jackson D (1953) a zone of stasis (ischemic middle zone) and an erythemal peripheral zone. Microscopy visualizes vascular thrombosis in the middle and peripheral zones.
The intensity of tissue heating (depth of damage) depends on the physical characteristics of the thermal agent (low-temperature, high-temperature), the method of heat transfer (conduction, convection, evaporation), and the heat-protective properties of clothing. The extent of skin damage depends not only on the actual temperature, but also on the time of its exposure, which is extended due to the fact that the skin has a fairly high heat capacity and thermal conductivity. The degree of tissue hyperthermia is directly proportional to the duration of heating. Short-term exposure to even very high temperatures may not lead to the development of burns. The higher the degree of tissue overheating, the faster cell death occurs.
Classification. Currently, our country uses the classification adopted at the XXVII All-Union Congress of Surgeons. The following degrees of damage are distinguished (Fig. 20. 1):
1st degree - superficial epidermal burn
2nd degree - burn of the upper layer of skin
Grade 3 - coagulation and necrosis of the entire papillary layer or deeper layers of skin.
3A degree - necrosis of the epithelium extends to the depth of the epithelial layer to the germinative layer, but does not completely cover the latter, but only at the tops of the papillae, skin appendages are preserved.
3B degree - necrosis extends to the depth of the entire epithelial layer and dermis.
4th degree - damage to deeper tissues (subcutaneous tissue, fascia, muscles, tendons and bones).
A classification that distinguishes four degrees of damage is widespread abroad:
— first degree – corresponds to the first degree of the domestic classification;
- second superficial degree - corresponds to degree II of the domestic classification;
- second deep degree - corresponds to IIIa degree;
- third degree - corresponds to IIIb degree;
— fourth degree – corresponds to IV degree.
Clinical picture.
Depending on the depth (degree of damage), burn injuries are characterized by various local clinical manifestations ( Table 20. 1 ).
1st degree burn is characterized by diffuse redness, swelling and severe soreness of the skin, and a local increase in its temperature. The thermal agent, due to irritation of the vascular nerves, causes intense vasodilation. After a few days, all manifestations disappear, leaving brown pigmentation of the skin. A typical example of a 1st degree burn is a sunburn.
With a 2nd degree , blisters filled with clear serous fluid form at varying depths in the thickness of the epidermal layer. The contents of such blisters are acellular serous fluid with a high protein content. Healing occurs due to the regeneration of the epithelium.
With a 3rd degree , the skin is blistered in places, spotted, with spots of a pale or dark shade, sometimes even black. Non-viable tissue forms a scab, which is torn away from living tissue to form a line of demarcation. If swelling is clearly visible in the burn area, then you can count on islet epithelization and healing without skin transplantation. Tender scars remain at the burn site.
3b degree burns, the entire thickness of the skin is affected, involving the superficial layers of subcutaneous tissue. The skin is pale gray in color, mottled, its sensitivity is reduced or absent. When healing occurs, rough scars form at the site of the lesion.
4th degree burns are characterized by deep tissue damage, often charring. Tissues turn into blackened, brittle masses. These burns cannot heal on their own.
The severity of the general condition of patients mainly depends on the area of the burned surface and the degree of the burn, the severity of which ultimately determines the prognosis of the disease. In the first days, the severity of the flow depends mainly on the area of the burned surface. The depth of the lesion affects mainly the further course of the disease.
Diagnostics
When diagnosing the depth of the lesion, it is necessary to take into account a complex of data obtained during the collection of anamnesis, examination of the victim and during diagnostic tests.
Anamnesis allows us to establish the type and duration of exposure to the damaging agent, factors that change the intensity of thermal exposure, and the presence of concomitant pathology.
During the examination, changes in the color of the epidermis and dermis, the presence and extent of edema, the presence of blisters and the nature of their contents, the presence of signs of circulatory disorders, the presence of tissue necrosis and its type are assessed.
During a physical examination, the state of pain sensitivity is determined: needle pricks, epilation test (hair pulling), tests with dyes.
Determination of burn area.
One of the important components of the diagnosis of thermal injury is determining the area of the lesion. The most convenient is to determine the area of the affected surface according to Wallace (A. Wallace 1951) - the “rule of nines”: head and neck - 9%, arm - 9%, leg - 18%, torso back and front 18% each, perineum, genitals - 1% (Figure 20.2).
Another common method is the "palm rule". According to research by J. Grazer (1997), the area of the palm of an adult is 0.78% of the total surface area of the body.
Local treatment of burns.
As first aid for burns, it is necessary to immediately stop exposure to the damaging factor, provide access to fresh air, cool the burned areas of the body (cold running water, cryopacks “Comprigel”, “Articare”, etc.), in case of extensive damage, administer painkillers (analgin, morphine , omnopon, promedol, moradol), apply sterile dressings to the affected surfaces. It should be noted that the key point in providing first aid is the rapid cooling of the burned surface, the correct implementation of which reduces the depth (degree) of the burn by one. Adequately performed first aid at the scene of an incident can reduce the risk of burn disease and reduce the number of complications.
Superficial burns of a small area are adequately treated on an outpatient basis, since in most cases they do not require surgical treatment. Various ointment dressings are used locally, which have a local cooling effect, protect the wound surface, stimulate healing, and prevent secondary infection. The most commonly used ointment sprays are “Olazol” and “Panthenol”.
In recent years, various wound coverings have been widely used in the treatment of borderline IIIA degree burns and deep IIIB-IV degree burns; perforated pig skin, xenoskin, has been successfully used for many years. The latter is placed on burn wounds, providing them with rest and protection from infection, without interfering with the cleansing of wounds and the simultaneous use of other drugs for local treatment.
Currently, there are two main ways to prepare deep burn wounds for autodermoplasty ( Table 20. 3. ): chemical necrectomy with delayed autodermoplasty and surgical necrectomy with simultaneous or delayed autodermoplasty. The tactics of local treatment using chemical necrectomy is quite justified for extensive deep burns of more than 40% of the body surface, provided that the general condition of the patients is extremely severe. Especially when treating elderly and senile patients, in whom severe concomitant pathology makes early surgical interventions impossible.
In these cases, from the first day after injury, local treatment should be aimed at the rapid formation of a dry burn scab, prevention of infection and deepening of burn wounds. For this purpose, cotton-gauze dressings with water-soluble ointments are used. This helps reduce fluid loss from the burn surface, warm the patient, form a dry scab, and does not require daily dressings.
In the following days, the formation of a dry burn scab is achieved by using wet-dry dressings. The optimal drugs during this period are also 1% solutions of iodopirone or iodovidone, which ensure drying of the scab and have a wide spectrum of antimicrobial and antifungal effects. It is also possible to use cotton-gauze dressings with water-soluble ointments. The use of fat-based ointments is contraindicated.
Treatment of the patient in an abacterial environment significantly accelerates the formation of a dry scab. In this case, an open method of treatment is used with the treatment of burn wounds two to three times a day with a 1% solution of iodopirone, iodovidone or the drug Naxol and the use of abacterial isolators or a Clinitron bed. Infrared irradiation of wounds helps dry out the scab. The formation of a dry scab reduces protein loss from the burn surface, helps reduce intoxication, and improve the general condition of the patient.
In case of deep circular burns of the extremities, when there is a high risk of compression and ischemia of the underlying tissues by the forming burn scab, with circular burns of the chest limiting its excursion, necrotomy is indicated in the coming days after the injury.
After the formation of a dry “mummified” scab, chemical necrectomy is performed using 40% salicylic ointment. The thickness of the ointment layer should be 1-2 mm. No more than 200 grams of ointment is used at the same time due to the risk of poisoning with salicylates, the level of which in the blood may exceed the permissible limit. After 48 hours, the burn eschar is bloodlessly separated from the underlying tissue. Taking into account this circumstance, chemical necrectomy can be carried out simultaneously on an area of up to 10-15% of the body surface.
After cleansing the burn surface from necrosis, to prepare the wound for autodermoplasty, it is advisable to use water-soluble ointments containing antibacterial drugs, possibly alternating with antiseptic solutions. Ultraviolet irradiation, monochromatic red laser light, and low-frequency ultrasound have a positive effect on the wound process.
If the area of deep burns of victims exceeds 10-15% of the body surface, it is advisable to perform the following staged chemical necrectomy at the same time and prepare granulating wounds for one-stage autodermoplasty on an area of up to 20% of the body surface. Such an operation is possible only with the use of a split perforated mesh autologous skin flap, which allows increasing the graft area in a ratio of 1: 2, 1: 4, 1: 6 or more.
In recent years, an increasing number of supporters have found a method of surgical excision of necrotic tissue. The leading method of treatment is early surgical necrectomy of burn wounds - radical excision of all affected tissues before the development of inflammation and infection, followed by simultaneous autodermatoplasty of skin defects. The operation is performed up to 5-7 days from the moment of injury directly to bring the patient out of shock.
In the structure of surgical treatment methods, the following are also used: early surgical cleansing of burn wounds - deliberately non-radical excision of the main mass of necrosis in order to reduce intoxication, delayed surgical necrectomy - radical excision of all affected tissues in case of developed inflammation and infection (performed 5-14 days from the moment of injury ), late surgical treatment of wounds (including surgical treatment of granulating wounds), amputation and disarticulation of limbs and their segments.
For third-degree burns, surgical necrectomy is performed tangentially (layer-by-layer) with a special instrument (dermatome, Gumby knife) until pinpoint bleeding appears from the layer of skin unaffected by the burn. For IV degree burns, surgical and necrectomy is often performed to the fascia with a scalpel or electric knife, followed by careful hemostasis. Early surgical necrectomy (tangential or fascial) with simultaneous autodermoplasty allows for deep IIIB-IV degree burns to restore the integrity of the skin within 3-4 weeks after injury on an area of up to 20% of the body surface.
It should be noted that the use of modern principles and methods of treatment of severe burn injury, including early surgical necrectomy with simultaneous subsequent autodermatoplasty (immediately after removing the patient from a state of shock), allows most patients to avoid the development of all further periods of burn disease, or to reduce the severity of its manifestations and consequences.
Currently, a new method of active surgical treatment of burnt patients using cultured allofibroblasts . The essence of the method is the use of allofibroblasts, artificially grown in laboratory conditions - connective tissue cells that determine the activity of regeneration processes, including epithelialization - for the plastic closure of burn wounds. They can be obtained from donor skin or cadaveric material; when cultivated, they are unpretentious and completely lose antigen specificity.
The method involves the transplantation of cultured fibroblasts onto extensive burn wounds of IIIA degree, donor wounds, including those that do not heal for a long time, or combined autodermoplasty using a culture of fibroblasts and mesh skin autoflaps, perforated in a ratio of 1: 6 and 1: 8 for deep burns IIIB- IV degree. The operation is preceded by chemical or surgical necrectomy.
Experience in surgical treatment of patients with extensive burns has shown that with borderline IIIA degree burns, wound healing occurs on average on the 8th day after transplantation of cultured fibroblasts.
BURN DISEASE. CLINICAL SYNDROMES
In burn disease, four clinical syndromes can be distinguished: Burn shock, Intoxication, Infection, Convalescence. There are no sharp boundaries between these syndromes.
BURN SHOCK. It occurs as a result of a neuro-reflex and neuro-endocrine reaction of the body. As a result of a strong inflammatory process in a burn victim, the central and peripheral blood supply is disrupted, the permeability of vascular and cellular membranes increases, the volume of circulating blood decreases with a violation of the ratio of its formed elements and plasma (hypovolemia), plasma escapes from the vascular bed and plasma loss through burn wounds. Plasma loss during burn shock depends on the depth and area of the burn.
Thus, with superficial burns, predominantly external loss of plasma is observed, and with deep burns, plasma enters the surrounding tissues and swelling occurs.
During a burn, the evaporation of fluid through damaged skin increases significantly, leading to a large loss of fluid from the victim’s body. Loss of fluid reduces the mass of circulating blood, resulting in a sharp deterioration in glomerular filtration of urine. Burn shock usually occurs within 2-3 days. Signs of burn shock include: an excited or inhibited state, in severe cases, consciousness is confused or absent; decreased pulse blood pressure, decreased amount of urine excreted by the kidneys (oliguria), vomiting, thirst, chills, muscle tremors.
INTOXICATION. As a result of the appearance in the victim’s body of toxic products, under-oxidized compounds, and bacterial tissue, a period of acute burn toxemia begins. Body temperature rises, loss of appetite occurs with the development of signs of toxic damage to internal organs (toxic myocarditis, hepatitis). During this period, it is necessary to carry out active detoxification measures (forced diuresis, plasmaphoresis, hemosorption).
INFECTION. At the third stage of burn disease, infection begins to progress. Metabolic disorders and weakened immunity give rise to infection of the body. Infection significantly complicates the course of the wound process - it maintains intoxication, suppresses restoration processes in tissues, and can affect various organs.
RECONVALESCENCE (recovery). It occurs from the moment of complete closure of granulating wounds. An important factor in recovery is prompt closure of burn wounds.
What happens to the skin during a burn?
The first symptom of a burn from household chemicals is sharp pain . Next, the tissues begin to break down and the skin color changes . It depends on the specific substance: it can take on a shade from white to brown. The border between affected and healthy tissues is always clearly visible.
The exact clinical picture of a chemical burn depends on the degree of tissue damage. There are four in total:
- First . The pain is mild or moderate. The tissues swell, turn red, and heat up.
- Second . The pain is moderate to severe. The surface of the skin turns red. Transparent bubbles form on it.
- Third. Sensitivity decreases. Large bubbles with cloudy contents or an admixture of blood are formed.
- Fourth . Tissues die. Necrotic areas of varying depths are formed.
The higher the degree of burn, the more severe the condition and the greater the risk of deep damage with subsequent formation of rough scars. Stages 1 and 2 can be dealt with at home. For grades 3 and 4, you should urgently seek medical help.
OBJECTIVES OF TREATMENT OF BURNS
FIRST AID FOR BURNS
The goal of treating burns is to preserve the life of the victim and restore the skin. In this regard, it becomes important to provide first aid:
- Stop the victim's contact with the damaging factor.
- Prevent microbial contamination.
ACTIVE TREATMENT OF A BURN
During further treatment, the doctor prescribes the following measures:
- Restoration of microcirculation to preserve the paranecrotic zone.
- Protection against infection and suppression of bacterial growth in the affected area.
- Excision of necrotic tissue.
- Stimulation of regeneration processes (granulation and epitilization).
- For dermal burns - surgical restoration of the skin.
Frostbite
Frostbite is damage to the skin under the influence of low temperatures, both from local freezing and from general hypothermia of the body. Low temperatures impair metabolism in cells and lead to their death.
1 Treatment of frostbite
2 First aid for frostbite
3 First aid for frostbite
Nature and degree of frostbite
A person can get frostbite in different situations:
- frostbite of the cheeks, nose, ears, fingers and toes in frosty weather;
- wearing tight and wet shoes at sub-zero temperatures;
- hypothermia of the body as a result of prolonged exposure to water or snow;
- prolonged exposure to the cold while intoxicated.
Watch for the following signs of frostbite. At first, a person will feel cold, then a burning sensation, first the skin turns red, and then turns white. Skin sensitivity is impaired and numbness occurs. Usually a hypothermic person does not feel his condition, and this makes diagnosis difficult.
Degrees of frostbite
Just like with burns, frostbite is divided into 4 degrees.
- 1st degree of frostbite : redness and numbness of the skin area and loss of sensitivity of the affected area of the skin, burning and itching occur. When warmed and rubbed, frostbitten skin begins to turn red. Stage 1 frostbite goes away within a week.
- Stage 2 frostbite is characterized by deeper damage to the layers of the skin and the appearance of blisters with clear liquid on the skin.
- 3rd degree of frostbite : tissue necrosis appears, healing takes place within a month with the formation of scars.
- 4th degree frostbite : not only the skin is affected, but also the bones and joints. The affected tissues are bluish in color and blisters appear.
EPLAN: PROTECTION, FIRST AID, TREATMENT OF BURNS
EPLAN - SKIN PROTECTOR
Eplan is able to penetrate the upper layers of the Epidermis, completely fill the free intercellular space of the Epidermis and create an additional barrier layer, which provides skin protection for a long time. Skin protection after treatment with Eplan lasts up to 8 hours.
EPLAN does not disrupt the intercellular connections of the stratum corneum of the skin, so the skin does not lose its strength and natural protective functions.
When EPLAN is applied to intact skin: EPLAN does not penetrate into the deep layers of the epidermis (Basal layer) and does not affect the natural proliferation of Epidermal cells, does not change the water-lipid balance of the skin.
EPLAN IS EFFECTIVE AT ALL STAGES OF BURN DISEASE.
EPLAN reduces pain in the burn site by blocking irritation of damaged nerve endings in the affected area, protects the skin after a burn from environmental influences and infection, and does not allow the body to lose fluid through the burn wound.
EPLAN reduces the flow of decay products of dead tissue into the victim’s blood and prevents intoxication. When treating large areas of burns, such as the treatment of burns with boiling water, steam, sunburn, the use of the drug does not lead to toxic damage due to the formulation itself - EPLAN is not toxic and does not contain hormonal components.
When treating burnt skin, EPLAN acts as an antiseptic, preventing infection of the burn wound (both for first aid for a burn and for protection against secondary infection), and eliminates skin itching.
FIRST AID AND TREATMENT OF BURN WOUNDS: EPLAN TASKS TO PREVENT INFECTION
EPLAN has high antimicrobial activity. The reason for this is the lanthanides that make up Eplan.
Phagocytosis is a process in which special blood cells and body tissues (phagocytes) capture and digest pathogens of infectious diseases and dead cells.
The phagocytic activity of blood leukocytes leads to rapid cleansing of the wound from pathogenic microorganisms: leukocytes begin to more actively destroy bacteria, and EPLAN does not interfere with the access of oxygen to the wound area. Thus, the use of EPLAN in the treatment of burn wounds can be considered as a drug for local enhancement of the patient’s immune status.
EPLAN is non-toxic, made without the use of antibiotics or hormonals. The use of the drug EPLAN becomes especially important in first aid for burns with boiling water and treatment of infected wounds with a large affected area. EPLAN is effective in treating the following injuries: treatment of burns with boiling water, steam, treatment of sunburn, thermal burn.
EPLAN IS A CATALYST FOR SKIN REGENERATION.
The effect of EPLAN as a drug for skin regeneration, skin restoration, rapid healing of wounds and burns is due to the presence of lanthanides in its composition. Lanthanides influence the process of cell proliferation. Application of EPLAN to damaged skin, a burn or a wound, triggers the process of lanthanide exposure to the membranes of proliferating skin cells, which leads to stimulation of their cell division. EPLAN cannot be considered as an inhibitor of kylon tissue activity, therefore its effect is local and has no aftereffect after use.
EPLAN WITH BANDAGE
Eplan-cream and Eplan-solution for the treatment of wounds and burns EPLAN WITH BANDAGE: maintains a moist environment and temperature of the wound, prevents the formation of a scab, provides access of oxygen to the wound, does not create obstacles to the removal of exudate from the wound into a dressing, prevents infection of the wound. EPLAN does not contain toxic components, antibiotics, hormonal or analgesic agents, and wound dressings with EPLAN allow the bandage to easily come off the wound without damaging injured healing tissue.
BEST WOUND-HEALING OINTMENT FOR BURNS EPLAN CREAM: TREATMENT METHOD
When the skin is locally exposed to temperatures above 55-60 degrees Celsius, aggressive chemicals, electric current or ionizing radiation, a BURN occurs. In assessing the severity of a burn, the area of the body surface affected by the burn is of great importance; there are 4 degrees of burns.
Degree I is characterized by damage to the most superficial layer of the skin (epidermis), consisting of epithelial cells. In this case, redness of the skin appears, a slight swelling accompanied by pain. After two to three days, these phenomena disappear on their own, and no traces remain after the burn, except for minor itching and flaking of the skin.
Stage II is characterized by the formation of blisters with a yellowish liquid against the background of redness of the skin. Blisters can form immediately after a burn or after some time. If the blisters burst, bright red erosion is revealed. Healing at this stage usually occurs by 10-12 days without scarring.
III degree burns are characterized by greater depth of damage with tissue necrosis (necrosis) and the formation of a burn scab. The scab is a dry, light brown to almost black crust; When scalded, the scab is soft, moist, and whitish-gray in color. There is a IIIA degree, in which the epithelial elements of the skin are preserved, which are the starting material for independent wound healing, and a IIIB degree, in which all layers of the skin completely die and the resulting burn wound heals through scarring.
IV degree burns are accompanied by charring of the skin and damage to deeper tissues - subcutaneous fat, muscles and bones.
Burns of I-IIIA degrees are considered superficial, and burns of IIIB-IV degrees are considered deep. It is possible to accurately determine the degree of burn (especially to distinguish IIIA from IIIB degrees) only in a medical institution using special diagnostic tests. In domestic conditions, thermal burns most often include: burns with boiling water, steam, iron, sunburn, etc. Burns and scalding with boiling water account for almost 40% of all deaths of children under 15 years of age. In a milder form, this is the most common type of injury for people of all ages.
How to treat burns with a burn remedy - EPLAN?
For first and second degree burns, we suggest using the drug EPLAN in ointment and liquid form. The affected area is lubricated with Eplan and, as it absorbs and dries, the treatment is periodically repeated until complete healing. If burn blisters occur, the exfoliated skin should be removed, but you do not need to open the blisters yourself before going to a medical facility, because this can lead to wound infection. Treat the edges of the wound with an antiseptic (hydrogen peroxide, miramistin, chlorhexidine), apply sterile wipes soaked in the drug and secure with a gauze bandage. Change dressings every other day. Epithalization begins on days 7-9, from the moment granulations appear. The treatment process under bandages is continued with EPLAN liquid (12-14 days). At the healing stage, the edges of the wound are treated with dry sterile wipes (without antiseptics).
If EPLAN is immediately applied to damaged areas, redness and inflammation disappear, and blisters with serous fibrous contents do not appear.
Features of electrical burns
The current penetrates inside the human body and forms a “loop”. The most dangerous are:
- Closed loop - when the current passes through the arms or legs.
- Bottom loop - the charge passes through the feet.
- Full loop - the current enters the body through the legs and exits through the hands.
It is impossible to say exactly what will happen after an electric shock. It all depends on the strength of the discharge and the characteristics of the person. Contact with an object energized by 240 volts is often accompanied by convulsions. It is impossible to unclench your fingers; the cable remains in your hand.
The danger of such interaction lies in the duration. When struck by a high-power electric current, a person is thrown away from the source, but severe burns appear, which are accompanied by charring.
SUNBURN. PREVENTION AND TREATMENT
TIPS FOR TREATING SUNBURN
When going on a trip, do not forget that the skin is defenseless against active sunlight, and the desire to quickly get a brown tan is understandable, but not entirely correct. The result of prolonged and uncontrolled exposure to the sun is a sunburn. This is characterized by poor appetite, sometimes vomiting, insomnia, fever, and tachycardia. Against this background, drowsiness may occur. Children suffer especially hard from sunburn.
What should you do to protect yourself and your family from sunburn?
Firstly, you need to actively moisturize your skin and drink as much water as possible, because the very first negative effect that solar ultraviolet radiation has is dehydration. Secondly, in the first hours after getting a sunburn, you can take antihistamines (suprastin, tavegil, etc.) - this will reduce skin inflammation and simple painkillers (ibuprofen, paracetamol) - this will reduce pain. Thirdly, use EPLAN burn ointment (or solution) to treat the affected area. Repeat the procedure 3-4 times a day. We recommend that you first lubricate the affected area with the solution in order to instantly relieve redness and swelling. EPLAN solution also has a cooling and analgesic effect. To consolidate the effect and soften the skin, we recommend continuing treatment of sunburn in the evening, using EPLAN cream. Fourth, to protect the skin from sunburn, we recommend applying Eplan solution to the skin 10-15 minutes before going out into the sun. Eplan forms a protective film on the skin, which will protect the skin from burns in the future.
Must remember! Changes in the structure of the skin are irreversible after any burn (including sunburn and boiling water burns); in the future, the skin may constantly react in a more severe form to new portions of sunbathing.
Detailed information on the use of EPLAN for the treatment of burns, wounds and skin lesions in the EPLAN section: AREAS OF APPLICATION
Treatment
If the injury occurs at home, it is most likely minor. Small areas of skin can be treated independently. The wound heals within a couple of weeks.
The affected area should not be treated with iodine or brilliant green, as they will aggravate the burn. It is better to use creams and ointments for healing burns, which include an antibacterial and antiseptic component. Preparations with sodium fusidine help avoid tissue rotting.
In the first week, you need to take especially careful care of the wound:
- daily smear the injury with an antiseptic solution, anti-burn creams, as prescribed by your doctor;
- carry out dressings regularly;
- for pain, use painkillers;
- antihistamines are required.
For treatment in a hospital setting, 2 treatment methods are used: medication and surgery.
Drug treatment
If a person suffers from high voltage, then most likely he will lose consciousness. In this case, a disruption of the heart rhythm and disruption of the cardiovascular system are possible. In this case, doctors send the patient to the intensive care unit. He is prescribed infusion therapy with anti-inflammatory and painkillers. In some cases, a blood transfusion may be required.
After stabilizing the victim’s condition, therapy is supplemented with local treatment for a speedy recovery. All creams and ointments that can be used to treat burns with blisters prescribed by doctors have an antibacterial effect and stimulate regenerative processes.
If the nervous system is disrupted as a result of an electric shock, the patient is prescribed sedatives and sometimes antidepressants. To stabilize the functioning of the cardiovascular system - stimulants. If circulatory disorders or cerebral edema are detected, then taking dehydration medications is recommended.
Surgical intervention
Surgical intervention is necessary only for the 3rd or 4th degree of severity of the injury. Surgeons clean the affected area and transplant healthy skin.
In particularly severe situations, amputation may be required. It is recommended for those patients whose injury is not amenable to conservative treatment methods and skin grafting.
The decision is made individually, based on the patient’s condition. In some cases, surgery is required immediately when there is a real threat to life or health. Sometimes doctors decide to postpone intervention until the patient has partially recovered, that is, they give time to recover from the shock.
FIRST AID FOR BURNS WITH BOILING WATER AND STEAM
A burn is an open injury or destruction of the skin and mucous membranes. For burns, not only the type of damage factor matters, but also the duration (exposure) of its action.
The skin is the outer covering that protects the body and its connection with the environment, its mass is 4-6%, and together with the subcutaneous layer - 16-17% of the total body weight, its area in average adults is approximately 1.7 m2 . The skin performs a number of important functions: protection from the external environment, thermoregulation, participation in metabolism, water and heat transfer, blood distribution in the body, receptor, secretory, pigment-forming, respiratory, energy-saving (fat depot), immune.
When burned by boiling water or steam, tissue damage occurs quickly; the source of the burn must be removed immediately. Cooling significantly reduces the severity of the burn and relieves severe pain.
Burns from boiling water and steam are a very important problem in adult and child traumatism: burns become especially dangerous for young children and the elderly due to imperfections in the body’s protective functions. Most cases of burn injury occur at home due to negligence.
A superficial burn with boiling water and steam, like a sunburn, should be immediately treated with an anti-burn remedy - EPLAN solution. This will allow injured skin to heal in the shortest possible time. The drug can be used in different age categories. In serious cases, when anatomically significant areas (face, neck, perineum) are affected by the burn, you should immediately consult a doctor.
Detailed information on the use of EPLAN for the treatment of burns, wounds and skin lesions in the EPLAN section: AREAS OF APPLICATION
Causes of electrical burn
When a person touches a bare wire, it completes an electrical circuit. Tumors and injuries occur at the site of entry and exit of the discharge. Sometimes there are disturbances in brain function and soft tissue damage.
Experts name several main factors that can cause a burn:
- Contact with a poorly connected socket.
- Contact with the device with a wire on which the insulation is broken.
- Old wiring.
- Contact with high voltage line.
- Lightning strike.
HOW TO USE BURN OINTMENT IN FIRST AID
There are several stages in providing medical care for burns.
First stage (prehospital)
includes first aid for burns, provided in the form of self- and mutual aid at the scene of the incident. The burn surface for superficial burns is painful, so mechanical cleaning is allowed only in case of severe soil contamination by irrigation with antiseptic solutions. It is necessary to choose the optimal remedy for burns in a particular case. Burn wounds are covered with anti-burn dressings that do not stick to the wounds or sterile dressings with water-soluble ointments (levomekol, levosin, dioxykol, dermazin).
Instead of traditional remedies used in these cases, we recommend the universal, ready-to-use drug EPLAN (ointment and solution). EPLAN has unique properties for providing first aid, especially for sunburn.
EPLAN has the following useful properties: - pronounced absorbent activity (dehydrating activity is 13.5 times higher than that of a hypertonic NaCl solution); -low toxicity; -good permeability in fabric; - no irritating effect; - ease of application on surfaces.
If the ointment (cream) is immediately applied to the damaged areas, redness and inflammation disappear, and blisters with serous fibrous contents do not appear.
For local treatment of burns with EPLAN, two methods can be used: open (without bandages) and closed (with bandages), subsequent dressings are carried out daily or every other day until the wounds are completely healed.
First aid
First of all, it is necessary to stop human contact with the current source. In this case, you need to be vigilant and take precautions. Rubber gloves are put on your hands, and shoes that do not have rubber or metal inserts are put on your feet.
Note! It is acceptable to use a wooden plank to push the person away from the source. In this case, you should stay at a safe distance from it. After the contact is suspended, it is important to turn off the switch and completely turn off the power supply.
If you notice that the victim’s skin color has changed at the site of contact with electricity, and he is suffering from severe pain, then you need to call an ambulance. To choose a treatment method, it is necessary to determine the duration of exposure to the electric discharge and the degree of damage.
First of all, it is necessary to stop human contact with the current source.
If after the cessation of contact the victim is unconscious, then his breathing and heartbeat are checked. If necessary, take emergency resuscitation measures - artificial respiration, cardiac massage.
Note! Your feet should be slightly higher than your head to restore your heart rate.
If the victim is conscious, but complains of pain, then an anesthetic can be given.
Examine the victim's body. The area of the burn is indicated by special marking points. If entry and entry points are clearly identified, a sterile bandage is applied to the affected area to prevent infection of the open wound. Small wounds can be washed under running water.
Providing first aid for electrical burns to a child
If a child has been injured, then calling an ambulance should not be neglected, even if it seems to you that the child’s burn is not severe.
If a child has lost consciousness, he must be kept warm. If there is no breathing, it is necessary to hold your nose and perform artificial respiration until it is restored.
Keeping electrical appliances away from small children and away from electrical outlets and components can reduce the risk of electric shock.
Burns in children, as in adults, are accompanied by severe pain. While waiting for an ambulance, you can give your child an approved painkiller.
Attention! It is forbidden to leave the victim alone, as emergency assistance may be needed.