An oral burn is damage to the oral mucosa through exposure to high temperature, chemicals, electrical or light radiation. This condition is extremely painful, as there are a large number of nerve endings in the mouth. The mucous tissue becomes swollen and red. Later, the burnt epithelium peels off and painful areas appear.
Treatment for a burn will depend on the extent of tissue damage and the area of spread of the injury. First of all, it will be aimed at neutralizing the cause of the injury and relieving the pain syndrome. Further treatment is aimed at preventing infection of the affected area and speeding up its healing.
Types of oral burns
A burn is a very common injury. Along with the oral cavity, the larynx and esophagus may be affected. There are four main forms of burns:
- Thermal burn. Occurs through contact of the oral cavity with hot liquid or steam.
- Electrical injury. The most common case of such an injury is a violation of the rules for conducting physiotherapeutic procedures.
- Chemical burn. This injury occurs as a result of contact of the oral mucosa with acids, alkalis or chlorine.
- Radiation burn. You can get such a burn during radiation therapy in the complex treatment of malignant neoplasms of the larynx.
Causes of burns and methods of preventing them
The most common cause of burns is contact of oral tissues with liquids or high-temperature steam. The oral mucosa turns red, swelling appears, and then the upper layer peels off. Electrical burns occur due to incorrect electrophoresis. The size of the lesion will correspond to the size of the electrode.
Chemical burns most often occur in children when trying to test household chemicals, but burns sometimes occur in the dental chair. This can occur upon contact with silver nitrate, solutions for cleaning the dental canal, etc. In case of a chemical burn, the severity of the condition depends on the chemical composition of the substance that has entered the mouth and the strength of its concentration. Ionizing radiation is used in radiation therapy and can also cause burns to the mouth and larynx.
It must be said that the method of preventing burns is basic caution. Drinks or food that are too hot should not reach the table. Steam inhalations for children under 14 years of age are extremely dangerous and do not have any therapeutic effect. As for chemical burns in children, household chemicals must be carefully isolated and have warning labels. Do not pour chemical solutions into other containers, especially drinking bottles.
Etiology, prevalence, pathogenesis
Post-intubation injuries of the trachea are understood as a violation of the anatomical integrity or functional state of the trachea that occurs after intubation. Military conflicts, urbanization, the increase in road traffic injuries, natural and industrial disasters increase the number of people in need of resuscitation measures. As a result, the number of patients with concomitant trauma who require long-term artificial pulmonary ventilation (ALV) and tracheostomy increases annually by 3-5% [37, 52, 68]. The need for long-term mechanical ventilation also arises after surgical operations in patients with diseases of the heart, brain, and abdominal organs [23, 26, 36]. The pathological condition of the trachea, which develops during prolonged intubation through the larynx or tracheostomy, is proposed to be called post-intubation disease [2, 36]. According to the literature, the frequency of injuries to the larynx and trachea accompanying long-term mechanical ventilation ranges from 14 to 80% [42, 44, 57]. The main ones are erosions and ulcers (50-80% of observations), granulations (up to 30%) and cicatricial stenosis [8, 17, 19, 39, 41]. The frequency of the latter varies very widely - from 0.2 to 25% [5, 9, 29, 33]. Such a serious complication as tracheoesophageal fistula develops in 0.5-5.4% of patients [7, 21, 35]. The main cause of damage to the larynx and trachea during intubation is mechanical impact on its wall. The literature considers two leading mechanisms of such damage. The first includes direct mechanical trauma to the larynx and trachea, caused by rough and repeated attempts at intubation, the use of rigid conductors, mismatch of the size of the endotracheal tube, its displacement inside the lumen of the trachea during coughing, barotrauma during jet ventilation, as well as significant overinflation of the sealing cuff of the endotracheal tube. In this case, the mucous membrane of the larynx and trachea often suffers, which leads to the development of fibrinous granulation laryngotracheitis. In rare cases, tracheal perforation or its complete rupture occurs with the development of mediastinitis [3, 30, 59, 61, 64, 66]. Perforation usually occurs in the membranous part of both the cervical and intrathoracic trachea. Longitudinal tears ranging from 2 to 13 cm in length are more often observed [26]. According to a number of authors [58, 63], the incidence of tracheal rupture during intubation ranges from 0.05 to 0.19%.
Another mechanism of damage to the larynx and trachea is impaired blood circulation in the mucosa associated with prolonged compression in the area of fixation of the inflatable cuff of the endotracheal and tracheostomy tubes, as well as along the edges of the tracheotomy wound. If the pressure on the tissue exceeds 25-30 mmHg, ischemia occurs in the mucous membrane and cartilage of the larynx and trachea, followed by inflammation and necrosis [2, 5, 19, 23, 26, 36, 44]. In the future, this can lead to their cicatricial stenosis.
An important factor causing damage to the tracheal mucosa with the formation of its scar deformation is the reflux of gastric and duodenal contents into the pharynx, followed by aspiration. More often, this complication occurs in patients with severe traumatic brain injury, accompanied by damage to the brain stem, central and peripheral respiratory disorders. In 75% of such patients, a significant decrease in cough and swallowing reflexes is determined, up to their complete loss, which leads to overflow of the airways with products of aspiration and bronchial secretion [15, 19, 45, 60, 62]. Aggressive contents can quickly cause inflammation of the intact mucous membrane of the larynx and trachea, aggravate damage to their walls in the area where the endotracheal tube is located with the addition of a productive component in the form of growth of granulations into the lumen of the organ and the development of chondroperichondritis [21, 62].
Great importance in the development of post-intubation complications is attached to bacterial inflammation, the rate of occurrence of which depends on the type of microorganism and the contamination of the larynx and trachea [44, 56]. On days 2-6 of mechanical ventilation, 36-40% of patients develop nosocomial pneumonia, and 6% develop pulmonary atelectasis. Bilateral endobronchitis of II-III degree is diagnosed when the duration of mechanical ventilation is more than 7 days in all patients [19]. The experiment found that acute bacterial inflammation of the mucous membrane, cartilage of the larynx and trachea provokes autoimmune aggression against these tissues, which leads to chronic inflammation and scar-fibrous deformation [1, 23, 34, 55]. M.A. Shuster and E.K. Onufriev [53] established that the autoimmune process is a delayed-type reaction to collagen localized in cartilage.
Considering that the long stay of the endotracheal tube leads to the obligatory development of chondroperichondritis of the larynx with the subsequent formation of cicatricial stenosis, patients in intensive care units and in need of respiratory support, especially if its duration is unpredictable, a tracheostomy is applied on the 3-5th day from the moment of intubation [11, 38-41].
Endoscopic diagnostics
Trophic damage to the wall of the larynx and trachea is determined by the duration of exposure to the endotracheal and tracheostomy tubes. The range of their visual manifestations ranges from minimal changes in the form of edema and hyperemia of the mucous membrane to maximum changes - the formation of a tracheoesophageal fistula [7, 8, 17, 35].
Most often, changes in the larynx and trachea during naso- or orotracheal intubation develop at the level of the vocal and subvocal parts of the larynx, in the cervical trachea at the level of fixation of the inflatable cuff of the endotracheal tube, as well as in the area of the distal end of the latter [3, 16, 18, 29, 54].
In the first 3 days of orotracheal intubation, catarrhal and erosive lesions of the mucous membrane of the anterior and lateral walls of the larynx and trachea predominate. Less commonly, the damage is circular in nature [8, 17, 23]. In 62% of patients, catarrhal and erosive laryngitis is detected [19]. Unilateral and bilateral paresis with degree II-III laryngeal stenosis were diagnosed in 23% of patients [41]. It is believed that laryngeal paresis is caused by swelling of the mucous membrane, prolonged limitation of mobility of the laryngeal joints due to the installed endotracheal tube, as well as its exclusion from respiratory and vocal function [8].
V.E. Kokorina [21] found that most often during orotracheal intubation the posterior wall of the larynx at the level of the tube cuff is affected - in 80.2% of patients on the 3rd day of mechanical ventilation. The author explains this localization by compression of this zone between the inflated cuff and the gastric tube and the development of ischemia. With a decrease in pressure in the cuff of the endotracheal tube, 28.8% of them showed epithelization of acute erosions within 24 hours.
On the 3-5th day of orotracheal intubation, 11-17% of patients develop ulcerations of the posterior part of the vocal folds, interarytenoid region and areas of the trachea in the area where the endotracheal tube cuff is located [19]. During these periods of mechanical ventilation, unilateral and bilateral paresis with laryngeal stenosis of II-III degree were detected in 31% of patients, proliferation of granulations in the subglottic cavity of the larynx - in 10% and in the cervical trachea - in 8% of patients [41].
When the duration of mechanical ventilation was from 6 to 10 days, post-intubation laryngitis was found in all cases, unilateral and bilateral paresis with laryngeal stenosis of II-III degree - in 46% of patients, proliferation of granulations in the subglottic region of the larynx - in 7% and in the cervical trachea - in 10% of patients [23, 41].
Orotracheal intubation lasting more than 10 days is accompanied by post-intubation laryngitis in all patients, unilateral and bilateral paresis with laryngeal stenosis of II-III degree - in 63%, proliferation of granulations in the subglottic region of the larynx - in 8%, in the cervical trachea - in 14% and in the thoracic trachea - in 4% of patients [23, 41].
After tracheostomy, damage to the trachea mainly develops along the upper edge of the tracheostomy and at two levels of the thoracic trachea - at the site of fixation of the inflatable cuff of the tracheostomy tube and along the lower edge of its position. Subsequent tracheal stenoses are localized there [10, 12, 16, 18]. Damage to the mucosa distal to the tube, as a rule, is a consequence of traumatization by the catheter during sanitation of the trachea and bronchi [8].
In the first 3 days after tracheostomy, catarrhal and erosive lesions of the tracheal mucosa predominate [8, 21].
On days 3-7 after tracheostomy, tracheal ulcers are found in 16.1% of patients. Superficial, round-shaped ulcerative defects with a diameter of 0.5 to 1.5 cm are detected along the side walls of the trachea at the level of the distal end of the tracheostomy tube. Their bottom is represented by a loose, dirty gray coating of fibrin. Tracheal ulcers, in contrast to laryngeal ulcers, are characterized by greater depth and size, progressive course and rapid development of granulations [2, 36].
Epithelization of these ulcers in most patients was observed within 28 to 42 days after tracheostomy. In a number of observations, hypergranulations were detected [36]. The growth of granulations was observed, as a rule, in the area of fixation of the inflatable cuff of the tracheostomy tube [41].
In the long term after prolonged tracheal intubation, 0.2-25% of patients develop cicatricial stenosis of the larynx and trachea [5, 9, 29, 33]. The location of the stenosis depends on the type of intubation, and the degree depends on its duration. During orotracheal intubation, the level of stenosis extends from the vestibular larynx to the cervical trachea. During intratracheal intubation (after tracheostomy), the cervical and thoracic parts of the trachea are affected. In 43-80% of patients, combined stenosis is detected [41, 43].
In some patients, intraepithelial granulomas of the larynx and trachea are detected within 14 days to 2 years from the date of intubation. During endoscopic examination, granulomas look like smooth, brightly hyperemic tumor-like formations with a poorly defined stalk, ranging in size from 0.5 to 1.5 cm [2, 19, 36].
Morphology
A morphological study of fragments of the tracheal wall obtained during the application of a tracheostomy revealed dystrophic changes already by the 1st-2nd day of mechanical ventilation. They were characterized by poor staining of the ground substance, impregnation of it with plasma proteins, and pyknosis of chondrocyte nuclei [23, 41].
By the 3rd day of mechanical ventilation, perichondrial detachment, usuration of the surface of the cartilage and fibrinous deposits on it were detected. Cartilage cells in the cartilage disappeared [19, 43]. Thus, already 3-day intubation caused pathological changes not only in the mucous membrane of the larynx and trachea, but also destructive and dystrophic changes in the tracheal cartilage.
By days 4-7 of mechanical ventilation, dystrophic and destructive changes in the tracheal cartilage progressed. There was no perichondrium in them, the surface of the cartilage was urinated, and foci of necrosis were identified. In some patients, replacement of cartilaginous tissue with granulation tissue was noted. Focal accumulation of leukocytes and hemorrhages were detected in the peritracheal connective tissue [19, 23, 41, 43].
With mechanical ventilation for more than 7 days, along with the death of cartilage and its replacement with granulation tissue, regeneration processes were detected, which was manifested by focal proliferation of chondrocytes, thickening and fibrosis of the perichondrium, as well as sequestration of dead cartilage [23, 43].
The results of histological examination of biopsy material from the tracheal mucosa obtained during bronchoscopy generally correlated with the data from studies of fragments of the tracheal wall taken during tracheostomy. In the bottom of tracheal ulcers that developed on days 3-7 after orotracheal intubation, necrotic masses and destructively altered leukocytes were determined, and in their edges - the presence of granulation tissue with leukocyte infiltration and detritus on the surface. When the defect existed for up to 21-35 days, 21.4% of patients developed squamous metaplasia of the epithelium, destruction or focal ossification of cartilaginous structures [36].
Morphological studies of biopsy material from the area of granulation stenosis on days 21–49 after orotracheal intubation or tracheostomy revealed granulation tissue with a vascular-poor stroma, consisting of macrophages and neutrophilic granulocytes, sometimes with areas of necrosis [2].
With the development of cicatricial stenosis in the period from 3 months to 6.5 years after long-term mechanical ventilation, excessive growth of connective tissue with lympholeukocyte infiltration around the glands in the submucosal layer was detected, and massive growths of coarse fibrous connective tissue were detected near destructively altered cartilaginous half-rings [2, 36].
Histological confirmation of the diagnosis of intraepithelial granuloma was the presence in the tissue of the formation of inflammatory sclerotic changes with neutrophilic leukocytes, macrophages and fibroblastic elements [36].
Thus, endoscopic and morphological studies have shown that prolonged tracheal intubation in combination with artificial ventilation initiates the formation of ulcerative tracheitis already on days 3-7. The existence of an ulcer for 2 months leads to excessive growth of granulations, destruction of cartilaginous structures and the formation of connective tissue in the submucosal layer and in the area of pathologically altered cartilage. The course of chronic inflammation and continuous stimulation of fibrogenesis for 3 months to 2 years lead to the formation of a stenosing tracheal scar.
Based on endoscopic and morphological studies D.V. Trishkin (2007) identified 4 clinical and pathogenetic variants of post-intubation tracheal disease: ulcerative tracheitis (4.6±3.2 days), granulation tracheal stenosis (36±9 days), cicatricial process in the trachea, presented in the form of inflammatory pseudotumors (9, 2±6.6 months) and cicatricial stenosis (4.9±3.6 months) [2, 36].
Endoscopic prevention and treatment
The indication for surgical treatment of stenoses that have developed as a result of complications of long-term mechanical ventilation is a violation of tracheal patency. The incidence of postoperative complications ranges from 6.2 to 28%; postoperative mortality, according to some data, can reach 10% [6, 43]. In this regard, more and more attention is currently being paid to the prevention of post-intubation complications. It primarily includes the treatment of early manifestations of post-intubation disease - erosions and ulcers.
One of the accessible and effective methods for preventing post-intubation injuries of the larynx and trachea is adequate sanitation of the trachea and bronchi. In this case, antiseptic substances and antibiotics are used, which are injected directly into the lumen of the trachea and bronchi [13, 24]. As an antiseptic, a 0.5-1% solution of dioxidine in a 2% sodium bicarbonate solution or a 0.01% solution of miramistin is often used [8, 17, 25]. If the patient has a large amount of mucopurulent secretion, 1-2 ml of a mucolytic (ambroxol, acetylcysteine, mistabron) is added to the sanitizing solution. If the patient is prone to bronchospasm, 5 ml of a 2.4% aminophylline solution is added to the injected solutions [26, 51]. However, this method has a number of disadvantages. Firstly, the method of introducing sanitizing solutions remains the same - through the lumen of the endotracheal and tracheostomy tubes, which eliminates the sanitization of the “dead” space formed by the glottis cranially, the tracheal cuff caudally, the walls of the trachea and the walls of the tube enclosed in it laterally [26]. Secondly, sanitation of the trachea and bronchi with an antiseptic does not affect the repair of ulcers and erosions, but only allows the removal of purulent secretions.
Among other therapeutic endoscopic methods used for erosive and ulcerative tracheobronchitis, laser photostimulation is the best known.
The use of a helium-neon laser during therapeutic bronchoscopy is described in the publications of E.V. Klimanskaya et al. (1988-1990), S.I. Ovcharenko et al. (1990) and V.X. Sosyury (1991) [51]. The authors noted good results in patients with chronic bronchitis and pulmonary suppuration due to improved sputum production, increased concentration of antibiotics in the bronchi and improved local immune defense of the respiratory tract. A good result of the endobronchial use of a low-intensity helium-neon laser in patients with erosive-ulcerative tracheobronchitis was obtained by N.E. Chernekhovskaya [46, 49, 50].
The effect of laser radiation is manifested by a multi-level effect on the body. There are changes in the rate of synthesis of protein, RNA, DNA, collagen, changes in oxygen balance and the activity of redox processes, changes in the membrane potential of the cell and the pH of the intercellular fluid, and improvement in microcirculation. The result of this is the formation at the body level of complex adaptive neuroreflex and neurohumoral reactions with activation of the immune system [20, 51, 65]. The therapeutic effect of helium-neon laser radiation is manifested by stimulation of epithelization of the mucosa in erosive and ulcerative injuries, normalization of lipid peroxidation processes, ensuring a physiological regime of tissue regeneration, limiting scarring processes and to a certain extent prevents the repeated excessive formation of fibrous tissue at the site of scar dissection [14, 22 , 27, 31, 46].
A fairly new method of treating erosive and ulcerative tracheitis is the endobronchial use of nitric oxide supplied from the Plazon apparatus through the endoscope channel [40, 61]. It has been established experimentally and clinically that the use of NO therapy leads to a significant acceleration of wound healing [4, 32, 67]. Nitric oxide activates the function of macrophages and fibroblasts and stimulates tissue regeneration [28, 47].
NOT. Chernekhovskoy et al. The possibility of re-epithelialization of tracheal ulcers under ozone therapy conditions was investigated [48]. In the experiment, the action of ozone caused acceleration of re-epithelialization and proliferation of the population of basal and immunocompetent cells, which in turn contributed to more rapid closure of the mucosal defect. The result of clinical trials was a decrease in edema, mucosal hyperemia and epithelization of ulcers in all patients [46, 48, 49]. An ozonated isotonic sodium chloride solution with an ozone concentration of 5 mg/l is injected under the mucosa into the edges of bronchial ulcers and additionally into the lumen of the trachea and damaged bronchus in an amount of 60-80 ml. It is also recommended to apply Ozonide oil to ulcers of the trachea and bronchi [46, 49].
In case of severe inflammation in the bronchi, intrabronchial immunotherapy with the immunomodulator T-activin is used in combination with the endolymphatic administration of antibiotics into the interbronchial spurs [46, 49-51].
Thus, at present, despite the improvement of endotracheal tubes, the frequency of post-intubation trophic complications in patients requiring long-term mechanical ventilation is increasing. Since these injuries are localized mainly at the level of the larynx, tracheostomy and tube cuff, it is impossible to detect them in a timely manner during bronchoscopy performed through the lumen of the tube. At the same time, there is successful clinical experience of local endoscopic treatment of purulent and erosive-ulcerative tracheobronchitis, which can be used in the early stages of trophic injuries of the larynx and trachea in patients undergoing long-term mechanical ventilation. In this regard, the task of improving endoscopic techniques for examining and treating patients with prolonged tracheal intubation in order to prevent the development of laryngotracheal strictures and tracheoesophageal fistulas becomes urgent.
Symptoms and classification of burn severity
Treatment and first aid will be carried out depending on the severity of the burn received. There are three degrees of oral burn:
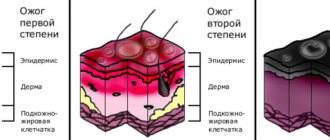
1st degree : the easiest. It manifests itself in the form of moderate pain, tissue redness and sometimes slight swelling. After eliminating the elevated tissue temperature, it goes away on its own and does not require further treatment.
2nd degree: moderate burn severity. Symptoms of the lesion: the appearance of tissue defects, plaque, tissue insensitivity at the site of the lesion. Intense pain requires anesthetics and is often accompanied by an increase in body temperature. If there is a burn not only to the mouth, but also to the larynx, then hospital treatment cannot be avoided.
3rd degree : the most severe. The entire epithelial layer to the deeper layers of the skin is deeply affected. This severity of burns is typical for chemical burns caused by hydrochloric acid and concentrated alkali.
First aid
A favorable outcome in treatment will depend on the speed of assistance, the nature and degree of mucosal burn. Initially, it is established what could have caused the injury. To do this, a visual examination of the room is carried out, the presence of a specific odor of the substance that caused the burn is taken into account.
If this does not give any result, then you need to examine the wound and the patient’s mucous membrane, carefully examine the vomit and the type of scab.
If the burn was caused by interaction with alkali, then the vomit will contain pieces of mucous tissue. When injured by iodine, they turn blue or brown. After a burn, a scab appears, the color of which can tell a lot:
- with acid burns it is yellow, that is, the injury occurred due to nitric or hydrochloric acid;
- for black - sulfuric acid, for white - hydrogen peroxide.
Once the agent that caused the burn has been accurately determined, measures can begin to eliminate the effect of this chemical. There are rules that should be remembered and followed immediately after a throat injury.
If the injury occurred as a result of boiling water or hot liquid, then the injured person should be given a glass of cold water to drink. To relieve pain, you need to give novocaine or lidocaine.
When injury occurs from various acids, it is necessary to give a lime mixture.
For alkaline burns - diluted citric acid.
The person must be provided with antiseptics and given a flow of fresh air.
If the burn is quite serious, it is necessary not to waste time, but to take the victim to the hospital, where doctors can quickly provide qualified medical care.
Treatment of oral burns
The most important thing in the treatment of burns of the oral cavity will be the provision of timely and high-quality first aid:
- For first-degree burns, rinse your mouth with cool, but not ice-cold, water for 15-20 minutes. If the pain is severe, you can take a painkiller.
- For second degree burns, rinse time with cool water is extended to 30 minutes. After this, the oral cavity is numbed with local anesthetics.
- If you have a third degree burn, you should wait for qualified help. In the complex treatment of such burns, antibiotics, painkillers and therapeutic aerosols are used to restore the epithelium.
In case of a chemical burn, it is important to immediately identify the chemical reagent and neutralize its effect:
- Alkali burns are neutralized by a slightly acidic rinse (citric acid solution);
- An acid burn should be treated with soap or soda solution.
The most important thing when treating burns to the oral cavity is to contact specialists as quickly as possible and provide high-quality first aid to yourself or the victim.
How does it manifest?
Doctors identify the following clinical symptoms that appear in a victim with a throat burn:
- Sharp pain in the throat, with a tendency to intensify when trying to swallow;
- Intense salivation;
- Nausea and vomiting;
- Cough syndrome;
- Pain localized in the chest area;
- Voice changes;
- Feeling of lack of air;
- Swelling of the cervical lymph nodes;
- A strong burning sensation in the palate;
- Hiccups.
In severe cases, a state of shock may develop. Even minor injuries can cause respiratory problems and cause suffocation, especially when it comes to a child or an elderly person.
Therefore, having identified the first symptoms characteristic of this injury, you should urgently provide first aid to the victim, then take him to a medical facility and transfer him to the hands of professionals.
Possible consequences
With this injury, patients are highly likely to develop complications and adverse consequences, which include:
- Chemical intoxication, poisoning;
- Collapse;
- Reflex cessation of breathing associated with damage to nerve endings;
- Scarring of the larynx, pharynx and esophagus area.