Skin and nail health
What is pityriasis alba? Causes of lichen alba Symptoms of lichen alba Diagnosis of lichen alba What can lichen alba be confused with? Treatment of pityriasis alba Doctor consultation on pityriasis alba Prevention
Skin rashes seem commonplace when you are young. Parents, children and teenagers get used to the fact that they have abrasions, acne, and insect bites. However, sometimes skin changes become a cause for concern. This occurs in cases where the nature of the rash is unusual and very persistent. Time passes, and such patients necessarily turn to a dermatologist.
What is pityriasis alba?
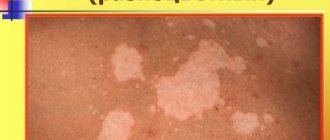
Lichen alba refers to diseases characterized by discoloration of the skin. Externally, pityriasis alba appears as the formation of milky white spots. The surface of these spots is no different from healthy skin, except for its shade. Lichen alba has clear boundaries. As for the size of the spots, it can range from a few millimeters to several tens of centimeters.
In most cases, the localization sites are areas of natural openings:
- Mouth;
- Eyes;
- Ears;
- Nostrils;
- Anus.
In addition, pityriasis alba can form on parts of the body that are subject to frequent friction:
- Elbows;
- Knees;
- Armpits.
Pityriasis alba can also appear on the outside of the feet and hands. Less commonly, white spots are localized on the mucous membranes. Scientists have noticed one feature of the manifestation of the disease - spots often form on parts of the body damaged by sunlight. White hairs often grow on white patches.
Other types of diseases can be found in the article, photos, signs and treatment of lichen in humans.
HERPES SIMPLE (HERPESIS SIMPLE)
This paper outlines the present-day concepts of the pathogenesis of herpes simplex, describes its main clinical manifestations, and considers its therapy. V.N. Grebenyuk, doctor med. Sciences, prof., head. Department of Pediatric Dermatology of the Central Research Institute of Dermatovenerology of the Ministry of Health of the Russian Federation. VN Grebenyuk, professor, MD, Head, Department of Pediatric Dermatology, Central Research of Dermatovenereologic Institute, Ministry of Health of the Russian Federation. P
Herpes growth is a serious medical and social problem. This is one of the most common human viral infections, often characterized by a persistent chronic course, affecting various organs, systems and tissues. According to WHO, about 70% of the population of our planet is infected with the herpes simplex virus (HSV) and approximately 10 - 20% of those infected have some clinical manifestations of herpes infection. HSV is a predominantly dermatoneurotropic DNA-containing virus; it also has tropism for other tissues, its size is 150 - 300 nm. The virion, in addition to DNA, consists of an icosahedral capsid and an outer shell containing lipids. It reproduces intracellularly (in the nucleus and cytoplasm) with a 14-hour reproduction cycle. During an acute infectious process, daughter virions are released from decaying cells. HSV infection can cause spontaneous abortions, fetal death and congenital deformities. The herpes virus is associated with the possibility of developing cervical cancer and some cardiovascular diseases. There are two antigenic types HSV-I and HSV-II, which cause lesions of the skin and mucous membranes of various localizations, which is determined by the place of introduction of the virus, usually through contact (coitus, kissing, through household objects). The source of infection can be not only patients with herpes, but also virus carriers who do not have symptoms of herpes.
| Rice. 1. Herpetic lesions of the face. a - forehead, eyelids, bridge of the nose; b - cheeks; c - lips and chin. |
3-4 weeks after infection, antibodies to HSV are formed in the body, the level of which remains relatively constant throughout a person’s life, regardless of the form of infection - manifest or latent. In the vast majority of people, the infection is asymptomatic or subclinical, and only in some infected people does it manifest clinically. Having penetrated the body, the herpes virus reaches a certain regional sensory ganglion (spinal or cranial) through lymphogenous, hematogenous or neurogenic routes, where it constantly persists. The latent state of the virus is based on the biological balance between micro- and macroorganisms. Under the influence of various provoking factors (psycho-emotional arousal, intoxication, overheating, etc.), a relapse of the disease occurs due to the reactivation of latent HSV, which leads to the formation of a recurrent disease. The range of clinical manifestations of the disease - from virus carriage to generalized forms - is determined both by the biological properties of the pathogen and the reactivity of the host. In most people, immune mechanisms, mainly cellular, maintain HSV latency. But in some infected people, antiviral resistance turns out to be untenable and relapses occur. There are two hypotheses that allow for the development of relapses based on both the static and dynamic state of the virus. According to the first hypothesis, the virus is located in the cells of the paravertebral sensory ganglion in an integrated or free non-productive state. Under the influence of the “trigger factor,” the virus, when activated, moves from the ganglion along the axon of the peripheral nerve to the epithelial cells, where it replicates. Cell susceptibility and weakened immune control are thought to contribute to this. According to the dynamic state hypothesis, replication and release of small amounts of virus from the ganglion occur continuously. Reaching the skin nerve, HSV causes microfoci of infection, which are restrained by defense mechanisms, which prevents relapses or weakens their manifestations. The development of relapses is also influenced by the state of local immunity. Its inhibition creates conditions for the replication of the virus that has reached the skin. The immune system plays an important role in containing the spread of herpes infection in the body. Immune protection is determined by the interaction and complex participation of specific and nonspecific factors. The main place in this system belongs to T-cell mechanisms of immunity. Mononuclear phagocytes and neutrophils play a significant role in maintaining local immunity and preventing the dissemination of infection. The protective functions of the body and the preservation of its homeostasis are also greatly influenced by the ability of cells to produce interferon.
Rice. 2. Herpetic felon.
| Rice. 3. Manifestations of herpes. a - on the palmar surface of the hand; b - on the thigh; c - on the buttocks |
Diseases caused by HSV are distinguished by a wide clinical variety of localization, severity, and characteristics of clinical manifestations. Primary herpes usually occurs after the first contact with HSV. More often it is observed in childhood against the background of a reduced immune status, in particular in the absence or low content of specific humoral antibodies. It is distinguished by the high intensity of clinical symptoms. The incubation period lasts several days. Primary herpes in newborns due to hematogenous dissemination becomes systemic, affecting the central nervous system and internal organs. The disease is characterized by herpetic lesions of the oral cavity, eyes, liver, bronchi, lungs, and brain. Usually the disease occurs acutely in the first days after birth and is manifested by anorexia, dyspeptic disorders, convulsions, septic condition, body temperature (39 - 40 ° C), disseminated herpetic rash on the skin and mucous membranes; Deaths are common in the first 2 weeks of illness. Children who have had generalized herpes experience neuropsychic complications. Kaposi's eczema herpetiformis is another severe type of herpes. Occurs mainly in children. It usually occurs in patients with atopic dermatitis, eczema, and other dermatoses in which there are skin lesions. The source of the disease can be patients with herpes in the acute stage. In adults, the disease may be associated with a recurrence of herpes labialis or another clinical form. Kaposi's eczema herpetiformis is characterized by a sudden onset (chills, malaise, body temperature up to 39 - 40 ° C for 1 - 1.5 weeks), a profuse vesicular rash on large areas of the skin, and painful regional lymphadenitis. The rashes appear in paroxysms over 2-3 weeks at intervals of several days. Often, along with skin lesions, the mucous membranes of the oral cavity, pharynx, trachea, and eyes are involved in the infectious process. Grouped and disseminated vesicles soon turn into pustules. In the center of the rash elements there are often umbilical recesses. After the crusts are rejected, secondary erythema remains on the vesiculopustules. Subjectively, the rash is accompanied by itching, burning, and soreness of the skin. Regional lymphadenitis is not uncommon. Patients are subject to hospitalization in an infectious diseases hospital or clinical hospital wards. In severe forms, the pathological process may involve the nervous system, eyes and internal organs. Relapses of Kaposi's eczema herpetiformis are rare, characterized by shorter duration and weakened clinical manifestations.
| Rice. 4. Genital herpes. a — bubble manifestations; b — erosive and ulcerative manifestations. |
The most common clinical form of primary infection is acute herpetic stomatitis.
It is more often observed in children in the first years of life; it is rare in adults. In weakened children, dissemination of the virus can lead to visceral pathology (in particular, hepatitis) and death. Acute herpetic stomatitis, occurring after about a week's incubation period, is characterized by a violent clinical picture. Chills, high body temperature (up to 39° C), painful vesicular-erosive rashes in the oral cavity, headache, general malaise, drowsiness - this is a list of the main symptoms of this disease. The rashes are most often located on the mucous membrane of the cheeks, gums, palate, lips, tongue, less often - on the soft and hard palate, palatine arches and tonsils, and spread to the skin around the mouth. The rash initially looks like grouped vesicles against a background of erythematous-edematous islands of the mucous membrane. The transparent contents of the elements become cloudy after 1 - 2 days, the covers of the vesicles are destroyed, and erosions form. In this case, regional lymph nodes are almost always enlarged and painful. Regression of the process usually occurs after 2 - 3 weeks. Recurrences of herpetic stomatitis, as a rule, are milder and resolve earlier. Herpes simplex is more common as a recurrent form. Clinical manifestations compared to primary herpes are less pronounced and not as long lasting. Most often, rashes are located on the face (lips, cheeks, nose), conjunctiva and cornea of the eyes, on the genitals and buttocks. The disease can last for many years and recur with varying frequencies - from several times a year to several times a month. In rare cases, the process becomes permanent when new rashes appear against the background of previous lesions that have not yet resolved. Frequent relapses of genital herpes are especially painful. The localization of herpetic lesions is determined by the site of virus introduction. The appearance of the rash is preceded by prodromal symptoms (burning, itching, tingling and other sensations). Grouped vesicles with a diameter of about 2 mm occur against a background of erythema. The transparent contents soon become cloudy and shrink into lumpy-yellowish crusts. When the vesicles rupture, scalloped erosions form. Their bottom is soft, reddish, the surface is smooth and moist. Regional, slightly painful lymphadenitis with a pasty consistency often occurs. The rash resolves within 1 to 2 weeks, leaving reddish-brown spots. When a microbial infection is added, the duration of relapses increases. Atypical forms of herpes simplex are known: abortive, zosteriform, disseminated, hemorrhagic-necrotic, migratory, elephantiasis-like, ulcerative, rupioid. The abortive form occurs in areas of the skin with a thickened stratum corneum and manifests itself as barely noticeable papules. Abortive manifestations of the disease also include erythematous and pruriginous-neurotic forms, characterized by local subjective disorders without typical rashes. The edematous form is usually located in areas of the skin with loose subcutaneous tissue (eyelids, lips) and is characterized by pronounced tissue swelling. Zosteriform herpes simplex is localized along the course of a nerve on the limbs, trunk, face and is accompanied by neuralgia, headache and general weakness. In the disseminated form of the disease, the rash simultaneously appears on areas of the skin that are distant from each other. The migratory form of recurrent herpes is characterized by a change in the localization of lesions. In hemorrhagic and hemorrhagic-necrotic forms, an admixture of blood is detected in the contents of the vesicles and necrosis develops. The elephantiasis-like form of the disease is characterized by severe swelling followed by the development of persistent elephantiasis in the affected area. Chronic cutaneous herpes simplex is an extremely rare clinical form. It is observed in patients with immunodeficiency and is characterized by permanent active manifestations of infection. Persistent ulcerative lesions up to 2 cm in diameter appear. The ulcerative form of herpes simplex is characterized by the development of ulcerative lesions, which is associated with a weakening of the patient’s immunobiological defense mechanisms and the increased virulence of the virus strain. This clinical type of herpes is characterized by the formation of ulcers at the site of weeping vesicles and fused erosions. The bottom of the ulcers is soft, pink-red in color, sometimes with a grayish-yellowish coating. In the first days of the disease, local pain and burning are expressed. Sometimes the rash is accompanied by inguinal lymphadenitis. The rupoid form of herpes simplex is usually localized on the face. It is caused by pyogenic infection with the development of cracks and layered crusts. Relapses occur several times a year. The rash is often accompanied by tenderness and enlargement of regional lymph nodes. With herpes of the hands, the process is often located on the distal parts of the hands. Limited lesions are represented by single dense blisters, accompanied by severe pain. The most common type of herpes simplex is facial herpes. In most people, these are sporadic focal vesicular eruptions, often resolving within 1 week. In severe cases, the process involves large surfaces of the face - nose, cheeks, forehead, skin and red border of the lips. Genital herpes occupies a significant place in the structure of herpetic diseases. Etiologically, its occurrence is equally often associated with types of HSV-I and/or HSV-II. Infection with one type of virus does not prevent the occurrence of HSV infection of another type, which leads to the formation of intermediate (“double”) antibodies. Mixed infection with HSV-I and HSV-II is quite common. The frequent isolation of HSV-I, which was previously considered the causative agent of non-genital forms of herpes, in genital lesions is due to the prevalence of orogenital contacts. Genital herpes is distinguished by the variability of its clinical picture and its tendency to have a chronic, relapsing course. In men, limited herpetic eruptions are often localized on the inner layer of the foreskin, in the head groove, and less often on the head and shaft of the penis. In women, the labia minora, clitoris, cervix, perineum and thighs are most often affected. Rashes (vesicles, erosions, ulcers, cracks) against a background of erythema and swelling are usually painful and are also accompanied by itching, a feeling of tension and heaviness in the perineum. About a third of patients have inguinal lymphadenitis. When the urethral mucosa is involved in the pathological process, serous discharge from the urethra and pain when urinating appear. The source of infection in the case of genital herpes is usually a patient in the acute stage of the disease; it can also be a virus carrier, given the possibility of asymptomatic persistence of HSV in the genitourinary tract in men and in the cervical canal. The incubation period for primary genital herpes lasts from one to several days. Clinically, primary genital herpes has a more severe and prolonged course. The localization of rashes on the genitals and adjacent areas is determined by the gates of the viral infection. A recurrent course of genital herpes is observed in the majority of infected people. Provoking factors are a variety of influences - psycho-emotional experiences, hypothermia, menstruation, weather and climate fluctuations, and other factors that disrupt the state of biological balance of the body, contributing to a decrease in the immune response and activation of HSV. The clinical picture, the amount of virus secreted by the patient and the associated infectivity are more pronounced with primary herpes than with a recurrent disease. Possible complications of herpes simplex: the addition of a secondary bacterial infection, reinfection with the released virus of other epithelial integuments, neurological manifestations (aseptic meningitis, transverse myelitis), encephalitis, disseminated infection of internal organs, psychosocial consequences (psychological instability). The risk of developing cervical cancer is 2 times higher in women who are seropositive for human papillomavirus types 16/18 and infected with HSV-II.
Diagnostics
The diagnosis of herpes simplex, especially its genital form, in most cases is based on the clinical picture. Difficulties arise with atypical manifestations of herpes. In this case, it is important to carefully collect anamnesis, paying attention to relapses accompanied by itching, burning, and ineffectiveness of antibiotic therapy. In addition, the patient may have a tendency to colds, general weakness, malaise, low-grade fever, and depression. Recurrent herpes is characterized by a wave-like course of the disease - an alternation of relapses and remissions. In women, relapses of herpes may be associated with certain phases of the menstrual cycle. The occurrence of erosions and ulcers on the genitals simulates syphilitic lesions. This similarity is most pronounced when a secondary microbial infection is attached, as well as during irrational therapy. The diagnosis of genital herpes is complicated by the fact that HSV is often associated with some resident autoflora microorganisms: chlamydia, streptococci and staphylococci, gardnerella and others, which can determine the occurrence of mixed infections. In addition, because herpes can be transmitted sexually, the patient must be tested to rule out other sexually transmitted diseases, including syphilis and AIDS. In complex cases, when clinical data is insufficient, laboratory diagnosis is possible. There are a number of specific laboratory tests to recognize HSV infection: isolation of HSV in cell culture, including HSV-I and HSV-II typing, tests to determine HSV antigen or DNA using polymerase chain reaction; serological tests - complement fixation test, ELISA, indirect immunofluorescence reaction, reverse passive hemagglutination reaction, protein-specific immune tests (immunoblotting), cytological examination (detection of multinucleated giant cells in scrapings from the lesion).
Treatment
Treatment of recurrent herpes remains a difficult task, which is not always solved effectively. It is possible to achieve some success if complex etiological and pathogenetic treatment is carried out at different stages of the disease, aimed, on the one hand, at suppressing the infectious agent, and on the other, at increasing the body’s immune reactivity. When choosing treatment, the stage of the disease should be taken into account. For relapses, interferon, antiviral chemotherapy, measles immunoglobulin, human normal immunoglobulin, levamisole, ascorbic acid, deoxyribonuclease, applications of 0.05% zinc sulfite solution are indicated; in the inter-relapse period - herpetic and polio vaccines, pyrogenal. The etiological focus is on antiviral chemotherapy drugs, which are more effective when used in the first hours and days of the appearance of rashes. Among them is the domestic drug Bonafton, which is used orally at 50–150 mg/day for 5–7 days for relapses. Simultaneously with the tablet form, 0.5% bonaftone ointment can be prescribed. It is applied to the lesions in an open manner when signs of relapse appear and is easily rubbed into the skin 2 - 3 times a day for 5 - 7 days. Side effects observed in some patients include malaise, loose stools, and dermatitis. Acyclovar (Zovirax) is effective, characterized by low toxicity and selectivity against HSV. The drug is used intravenously, orally and topically. It gives a pronounced therapeutic effect for Kaposi's eczema herpetiformis. Acyclovir is administered intravenously at the rate of 20 mg per 1 kg of body weight per day. However, the drug does not prevent herpes from recurring, infecting newborns, or infecting other people. Treatment of patients with recurrent herpes with acyclovir 0.1 - 0.2 g 5 times a day for 5 days during relapses shortens the time for resolution of rashes, reduces the severity of subjective sensations, smoothes out clinical manifestations and reduces the degree of virus shedding. Prophylactic administration of the drug 0.1 - 0.2 g 4 times a day for 6 - 12 weeks reduces the duration of relapses and weakens clinical manifestations. Other chemotherapy drugs: famciclovir, alpizarin (2 and 5% liniment), Viru Merz Serol, 1% oxolinic ointment, hevisos, ribavirin (virazol). A certain therapeutic effect is provided by immunocorrective drugs (myelopid, poludanum, arbidol), used both as monotherapy and in complex treatment. Myelopid (0.003 g in 2 ml of saline) is administered intramuscularly once every 3 days (5 injections per course). Treatment is carried out in two courses with an interval of 7 - 10 days. Poludan is administered subcutaneously into the forearm every other day, 100 mcg, for a course of 1000 mcg. Arbidol is prescribed 0.2 (2 tablets) 3 times a day - 5 days with a 2-day break, and then 0.1 g (1 tablet) 1 time per week for 3 weeks. Sodium nucleinate is also used orally at 0.5 - 1 g / day in 2 - 3 doses daily for 2 - 4 weeks. Taktivin is used to stop relapses and for prophylactic purposes. The drug is administered subcutaneously at a dose of 100 mcg every other day, 8 - 10 injections. During the inter-relapse period, 50 mcg is prescribed every other day, a course of 5 injections is repeated every 3-6 months. A course (4 - 5 injections) of treatment with timoptin is also carried out, which is administered subcutaneously at 100 mcg every 3 - 4 days. The courses are repeated after six months.
External treatment
Antiviral ointments, creams, lipsticks accelerate the epithelization of erosions, reduce or reduce subjective sensations in the affected areas. Local use of one or another antiviral drug in the treatment of herpetic lesions for 5 - 7 days shortens the time of regression; use 2 - 3 times a week during the inter-relapse period allows to prolong remission. Interferon has an inhibitory effect on HSV, which is applied to the skin and easily rubbed in for 4 to 7 days. During treatment, it is advisable to alternate antiviral drugs during relapses. Human interferons are effective in the treatment of recurrent herpes in the prodromal period and when the first signs of relapse appear. The ointment is applied to the lesions 2-4 times a day and rubbed in lightly; treatment is continued for a week. The use of interferon ointment during the inter-relapse period prolongs remissions and interrupts the development of relapses. In order to prevent relapses in frequently recurrent forms of herpes, patients for whom treatment is ineffective are prescribed a herpetic vaccine. Contraindications to its administration are lesions of parenchymal organs, diabetes mellitus, stage II and III hypertension, decompensated heart failure, acute infections and allergic diseases. The drug is administered intradermally during the period between relapses, 0.2 - 0.3 ml into the area of the flexor surface of one of the forearms. The first 5 injections are given after 3 - 4 days, the next 5 doses are administered after a 2-week break (once every 5 - 7 days). These 10 injections constitute the main course of treatment, 3–6 months after the end of which 1–2 cycles of revaccination are carried out, each of 5 injections with an interval between injections of 7–14 days and between cycles of 6–8 months. Over the next 2 years, an additional revaccination cycle of 5 injections is carried out every 8 - 12 months. At the injection site, after 18-24 hours, a local reaction develops, manifested by the development of erythema with a diameter of 2-5 cm with a papule in the center and accompanied by a burning sensation. During vaccination, a focal reaction such as abortive relapses may be observed. In this case, a break is taken in the treatment for 2 - 3 days, then it is continued. Specific vaccine therapy leads to an increase in the duration of remissions, a reduction in relapse periods, and the disappearance of subjective sensations. For the purpose of secondary prevention of relapse of herpes, the factors that provoke the disease are controlled. Great importance is attached to the sanitation of the body and health-improving measures in the process of medical examination.
Literature:
1. Barinsky I.F., Shubladze A.K., Kasparov A.A., Grebenyuk V.N.M.: Medicine. 1986, 269 p. 2. Masyukova S. A., Rezaikina A. V., Grebenyuk V. N., Fedorov S. M., Mkhitaryan A. G., Kolieva M. Kh. Immunotherapy of recurrent herpes simplex. Sexually transmitted diseases. Information analytical newsletter. Sanam Association 1995, 3, 27-30. 3. Minde CA. Genital Herpes. A guide to pharmacological therapy. Drugs 1994;47(2):297-304. 4. Whatley JD, Thin RN. Episodic acyclovir therapy to abort recurrent attacks of genital herpes simplex infection. J Antimicrobial Chemotherapy 1991;27:677-81.
Lichen alba in humans
The main causative agent of pityriasis alba is the Malassezia fungus , which occurs in 10% of the total population. This fungus does not cause any particular harm to humans. The affected areas are not accompanied by irritation and itching. In rare cases, lichen spots may rise above the underlying level of the skin and become slightly flaky.
When the spots peel, itching may occur, and if the lichen appears in winter, this may be accompanied by an inflammatory process. Lichen alba has the ability to change the pigmentation of the skin, as it creates obstacles to the penetration of sunlight and the detection of melanin. It is for this reason that even on a tanned skin surface it is difficult not to notice whitish spots.
Photo
Types of pityriasis
Pityriasis alba
It is only one type of pityriasis. It is characterized by damage to the scalp.
Pityriasis rosea
The most common form of pityriasis. Pink spots are localized throughout the body, have clear boundaries and a small depression in the center. The rash does not merge with each other, however, the elements tend to grow, which then ends in peeling of the skin around the spot.
Pityriasis rosea is characterized by severe itching. When combing the formations, white scales stand out clearly.
The rash normally goes away after 7 days, but with reduced immunity, frequent bathing, increased sweating and allergies, the healing process may slow down.
Pink pityriasis causes intoxication of the body, which is accompanied by an increase in body temperature and enlarged lymph nodes.
Lichenoid pityriasis
Another form of pityriasis is lichenoid pityriasis. It is characterized by the appearance of papules or vesicles on the skin, which form scales and resolve with scars.
There is acute lichenoid pityriasis, which is characteristic of childhood, and chronic, which is observed more often in adults.
Features of white lichen in a child
Pityriasis alba is also a very common skin condition among children. If your child suddenly develops pityriasis alba, do not immediately panic.
As a rule, this lichen goes away on its own . But despite this, the child should be shown to a specialist. The appearance of pityriasis alba occurs in the summer, which is characterized by high sun activity, or, conversely, in the winter due to the effect of cold air on the baby’s body.
Photo
Here you can see what other types of lichen look like.
During pregnancy
Pregnancy is associated with changes in hormonal levels and a weakened immune system, so during this period a woman may be faced with various kinds of previously undetected ailments. Lichen simplex can also be classified in this group. White spots may be the body's reaction to allergens. Perhaps the bacteria were already in the body and simply became active at a certain moment.
Lichen alba does not pose a threat to either the woman or the fetus. The only possible discomfort is itching. And if a woman experiences discomfort, this will affect her emotional state, which, in turn, will affect the child’s condition. Therefore, if inconvenience occurs, you should still get rid of lichen.
There are no contraindications for the treatment of lichen during pregnancy. Perhaps you should hold off on taking herbal teas internally: some herbs have a negative effect. But swimming in warm water will even be useful.
Who is susceptible to pityriasis alba?
As mentioned earlier, every tenth inhabitant of the planet is exposed to this type of lichen. However, among people there is a group that is most susceptible to developing pityriasis alba.
This group includes the following persons:
- People prone to frequent allergic skin rashes.
- People who frequently suffer from attacks of hay fever.
- People who once suffered from eczema or currently suffer from it.
- People who suffer from respiratory diseases based on allergic factors. This includes bronchial asthma.
Traditional medicine recipes for the treatment of asbestos pityriasis
Tincture of celandine helps well with pityriasis. This medicine can be bought in pharmacies, or you can prepare it yourself at home.
Several ways to lubricate affected areas of the body
- Celandine in vodka. It is necessary to collect celandine during the flowering period and dry it, fill the jar tightly with it and fill it completely with vodka. Leave the product in a dark place for three weeks, then strain it and fill it halfway with vodka again.
- Water tincture of celandine. Take 1 tbsp. spoon of dried celandine and pour a glass of boiling water. The vessel needs to be covered and left to steep for about 30-40 minutes. After straining, the tincture is ready for use.
A local remedy for skin diseases is a mixture of talc, zinc oxide, water and glycerin. This mixture has a calming effect and disinfects the skin, which has a positive effect on recovery.
To wash areas of skin affected by pityriasis, use the water in which buckwheat porridge was cooked.
The use of compresses made from raw yeast dough, which are applied to the rash, is encouraged.
When itching, it is important not to scratch the affected areas of the skin. Otherwise, the risk of developing an infectious process increases, which will significantly reduce the speed of recovery and threaten complications. To control yourself at night, you can apply bandages to the itchy spots.
You can use apple cider vinegar to relieve itching. Compresses made from a soda solution (1 teaspoon of soda per 1 glass of clean filtered water) and chamomile decoction will also be effective.
Causes
At present, the exact causes of pityriasis alba have not been established. Doctors say that the darker a person’s skin, the greater the likelihood of developing pityriasis alba.
Lichen alba in most cases occurs due to:
- Constant stressful situations
- Existing chronic organ diseases
- Intoxication
- Skin contact with synthetics
- Physical damage to the skin
Pityriasis alba often occurs in people who:
- Have thyroid disease
- Suffer from dysfunction of the pituitary-gonad system
- Suffer from increased blood clotting
- Suffering from anacid gastritis
- Suffer from atherosclerosis of the vascular system
- Suffer from asthenia and nervous system exhaustion
Reasons for development
Versicolor versicolor is a type of fungal skin infection that affects the stratum corneum of the epidermis and hair follicles. Its causative agents are two types of fungi, and infection is possible only through prolonged and close contact with the patient. And in this case, provoking factors play a big role. These include:
- weakened immunity;
- hyperhidrosis;
- disruption of the sebaceous glands;
- diseases of the endocrine system (obesity, diabetes, Itsenko-Cushing syndrome, etc.);
- hormonal imbalance due to pregnancy, menopause or taking hormone-containing medications;
- vegetative-vascular dystonia;
- abuse of antibacterial personal hygiene products;
- excessive exposure to ultraviolet rays (intense tanning, frequent visits to the solarium) and regular overheating of the body.
It is noteworthy that patients with pityriasis versicolor over 60 years of age are extremely rare. This is due to natural age-related changes in the skin, which make it less susceptible to pathogens.
In children under 10 years of age, the main causes of pityriasis versicolor infection are neglect of personal hygiene rules or improper skin care. At this age, with the protective functions of the skin intact, the body independently copes with pathogenic microorganisms attacking it, so the development of the disease does not occur. But closer to adolescence, when hormonal changes begin, the body’s susceptibility to bacteria, viruses and fungi increases, so children over 10 years old become infected with pityriasis versicolor just like adults.
Symptoms of white lichen
The symptoms of pityriasis alba are very pronounced, so they are very difficult to miss. But if you look at it from the other side, without special research it is difficult to say about the presence of this particular disease, since it has not yet been fully studied.
You might be interested! Ringworm in children: types, first signs and treatment
That is why, at the first suspicion, it is very important to contact a specialist who can conduct an examination and identify an accurate diagnosis.
The main symptoms of the presence of pityriasis alba:
- The presence of whitish spots, which most often appear on the cheeks, neck, thighs, shoulders, knees and elbows.
- The spots are very different in color from healthy skin.
- When you press on the stain, it does not change its shape or shade.
- No pain in the affected areas of the skin.
- The appearance of itching in children in the area where spots appear.
- The spots have unclear boundaries.
- The borders of the white spots may peel a little.
What is erythrasma
Erythrasma is a chronic bacterial disease affecting the epidermis layer in the deep folds of the skin. It is characterized by a long course - in some cases, symptoms develop for at least 10 years, without causing significant discomfort to the patient. The clinical picture of erythrasma is similar to a fungal infection of the skin, but modern dermatology classifies it as a group of pseudomycoses.
The following main stages are distinguished in the development of the disease:
- Progression. The first characteristic spots appear on the skin, their size slowly increases, and additional symptoms develop. In some cases, secondary infections occur. The spots gradually merge with each other, forming large areas of damage.
- Stabilization. New spots do not appear, and existing ones stop growing. Peeling of the skin begins. This stage is usually associated with a change in external conditions, for example, cold weather, during which the intensity of sweating decreases and the skin condition stabilizes.
- Exacerbation or relapse. Usually associated with the beginning of the warm season. But in the case of prolonged erythrasma, the disease constantly develops in waves, and after a slight decline its symptoms again actively appear.
- Remission. Occurs with a favorable microclimate, compliance with preventive measures and proper skin care. The color of the affected areas gradually returns to normal, itching and flaking disappear, and the skin is restored.
Without timely, well-chosen treatment, erythrasma can lead to the development of serious complications.
For example, it can provoke eczema and secondary infection in patients with diabetes or obesity. Also, the course of the disease is aggravated by increased humidity and contamination of the affected areas. As a result, its typical symptoms are complicated by burning, itching and pain.
Diagnostics
Diagnosis of white lichen, first of all, consists of taking into account the external manifestations of the disease. If a person has very fair skin, then the white spots on the body may be almost invisible. In this situation, the patient's skin is examined using a Wood's lamp .
A biopsy of the lichen spot can reveal the absence of pigment cells. But it is also worth noting that their presence cannot rule out the diagnosis. Lichen alba must be differentiated from secondary hypochromic changes, which can occur in the presence of certain skin diseases.
Solar lichen: causes and symptoms of the disease
29.01.2021
In summer, most people like to lie in the sun. Sometimes, after lying down like this, strange white spots appear on the body. They begin to peel off. What is this and what causes it?
This disease is called solar lichen . The causative agents of the disease are fungal microorganisms that live on the skin. In their normal state they are harmless.
After prolonged exposure to the sun, the fungus becomes active and affects areas of the body. The skin is affected mainly in the warm season.
This disease, which is classified as dermatological, is not considered contagious. A person can be a carrier of the fungus but not have symptoms of the disease.
The main causes of the disease:
- problems with the vegetative-vascular system;
- problems with the endocrine system and excess weight, diabetes ;
- frequent colds;
- problems with the liver and bile ducts;
- increased sweating;
- synthetic clothing;
- love for solariums;
- using sunscreen;
- lack of personal hygiene;
- use of drugs that weaken the immune system .
If you have sun lichen, you should not expose your body to tanning, as this can cause an exacerbation of the disease.
Symptoms of the disease are visible to the naked eye; it is indicated by the appearance of asymmetrical spots with uneven edges. Their color may vary. This is the first stage of the disease.
After some time, the spots may darken and merge into one whole. They will be conspicuous because the tan does not stick to them. This is already the second stage. The spots do not become inflamed, red, or swollen, but scales form on them, causing itching. If you scratch them, they begin to peel off.
Spots appear mainly on the chest , back , sides, stomach , and neck . In children and adolescents, the main places of localization are the head, lower and upper limbs, and armpits.
Solar lichen is considered a beach disease, so at the first symptoms you need to stop being in the sun. This disease has a fairly long incubation period, which can last from two weeks to three months. lichen appears in both autumn and winter.
To make a correct diagnosis for this disease, the doctor needs to conduct a thorough visual examination of the skin. In addition to the examination, it is necessary to undergo a general blood and urine , and blood biochemistry tests. And only after that the doctor will prescribe treatment.
A stool test may be required . Also, if necessary, special studies are carried out in the form of the Balzer iodine test, when a little iodine is applied to the lichen . If it really is ringworm , it will change color to brown. Another examination is carried out using fluorescent lighting. The light stream is directed onto the formed spot. If it changes its color and turns green or red, then the diagnosis is confirmed. The test for the presence of Beignet's symptom involves scraping off the top layer of the epidermis. The results are compared with the symptoms of leukodermatitis, leprosy, Gibert's disease, syphilitic roseola, and a diagnosis of solar lichen .
To avoid becoming the owner of solar lichen , prevention is needed. To avoid getting burns, take sunbathing in the morning and evening, use a protective cream, wear clothes made from natural fabrics, do not visit the solarium, and eat fresh fruits and vegetables. Do not use antibacterial soap or gel constantly, watch your heart and blood vessels .
Solar lichen does not stain, although it is not dangerous, so treatment should be timely.
Published in Dermatology Premium Clinic
Treatment
Treatment of white lichen consists of local therapy using creams, ointments and special solutions. These medications help restore normal skin pigment and contribute to the complete disappearance of spots. Most often, pityriasis alba is treated with hydrocortisone ointment.
Hydrocortisone ointment also treats dermatitis in acute forms, for example, venous. Here you can visually evaluate a photo of dermatitis on the legs.
Treatment of lichen alba should be resorted to in the following cases:
- If the whitish spots with lichen are widespread.
- If spots occur on the face and open areas of the skin.
- If white spots have formed against the background of acute dermatosis. This significantly worsens the general condition of a person.
- If there is a secondary infection.
- If there is scratching and severe itching.
How to treat pityriasis alba in a child:
- Washing the child with warm water without soap.
- Taking warm baths with soap containing glycerin.
- Using cream and ointment to moisturize the skin.
- Sun protection in summer.
- Treatment with creams and ointments containing corticosteroid hormones.
In addition, treatment of white lichen can be organized using traditional methods:
- Apply St. John's wort, sea buckthorn or peach oil to white spots.
- Use an infusion of calendula flowers and vodka to smear whitish spots (proportion 1:5).
- Spreading onion juice.
- Spreading with a paste of crushed sorrel and sour cream.
Treatment of erythrasma
To diagnose a patient with erythrasma, a dermatologist first uses a visual examination. This is especially true for rashes in the groin area, which have characteristic distinctive features in the form of pronounced protrusions and bubbles along the edges. Also, the affected areas of the skin are illuminated with a Wood's lamp and a microscopic examination of the scraping is performed to exclude other diagnoses: pityriasis versicolor or pityriasis rosea, candidiasis, dermatitis or eczema.
Treatment of erythrasma is primarily based on the use of antibacterial ointments that are used to treat the affected areas of the skin.
Under their influence, corynebacteria die, and the spots gradually lighten, decrease in diameter and disappear. On average, such therapy takes at least 7-10 days. Used in parallel:
- Antiseptics. Treatment with them is carried out before applying antibacterial ointment, as well as after it, to maintain dryness of the affected areas and prevent re-infection.
- Antifungal drugs. They are prescribed together with antibacterial drugs, since corynebacteria are similar in structure to fungal micelles.
- Exfoliating ointments. They help cleanse the skin of a layer of dead cells, activating its regeneration.
- Ultraviolet irradiation. Promotes skin disinfection and restoration. Patients benefit from both natural sunbathing and physiotherapeutic UV irradiation.
If the disease has not reached an advanced stage, the use of external medications is sufficient to solve the problem. But in some cases, with multiple skin lesions, to obtain the desired result, patients are prescribed systemic antibacterial therapy.
Prevention
To avoid the appearance of pityriasis alba, you must follow the following preventive rules:
- Compliance with personal hygiene rules.
- Use of personal hygiene items.
- Do not lie on the beach without a blanket and do not walk barefoot on the sand.
- In summer, do not be under the sun between 11 and 16 hours.
- Application of sunscreens and lotions.
- Dry your body thoroughly after bathing.
- Do not wear things made of synthetic fabrics.
- Include foods containing various vitamins and copper in your diet.
Complications and consequences
The disease itself does not pose any danger, except that its course may last for several years. If there are few spots, they do not have a bright, pronounced color and do not cause inconvenience to a person, no measures can be taken to treat them. The only thing to remember: if the immune system is weakened, allergies develop, or excessive exposure to sunlight, a relapse of the disease may occur.
Therefore, if you do not want to ruin your vacation or darken your mood with disrupted plans, then it is better to contact a specialist. Treatment will not take much time, but the spots can make themselves known as pronounced white lesions at any time.
As for complications, if personal hygiene recommendations are not followed, signs of an inflammatory disease may be added to lichen alba, the treatment of which will be more serious.