Lichen squamosus or psoriasis is a severe non-contagious skin pathology of a non-infectious nature, mainly localized in the area of large joints. It cannot be completely cured. Therapy is carried out to alleviate the chronic course and eliminate the manifestations of the disease. According to statistics, 4% of the world's population suffers from the disease.
Important: the disease can progress asymptomatically for a long period of time, after which it manifests itself due to hormonal imbalance, decreased immunity, stress, and other circumstances.
What is unique about the treatment of lichen planus at the GK Clinic?
At the GK Clinic, dermatologists will assess the course and spread of your disease and, taking into account your related diseases, will select the local, systemic or phototherapeutic treatment that is suitable for you.
In our Outpatient Center for the Comprehensive Treatment of Lichen Squamosus, you will undergo the necessary diagnostic procedures (biopsy to confirm the diagnosis, blood test before prescribing systemic PUVA therapy). After determining the clinical form of lichen planus and the spread of the disease, appropriate local treatment will be prescribed, which will then, during visits to the GK Clinic, be adjusted depending on the course of the disease. We will also select skin care products that are best suited for lichen planus. By prescribing appropriate treatment and skin care products, the course of the disease can be successfully controlled.
Psoriatic triad
During the examination, if the doctor is faced with the task of confirming or denying psoriasis, the specialist assesses the presence of signs of the psoriatic triad:
- stearin stain phenomenon - when scraped from the surface of the stain, soft whitish scales separate;
- the phenomenon of psoriatic film - when the scales are scraped off, the pink smooth surface of the plaque is exposed;
- the phenomenon of pinpoint bleeding - when the papules are completely scraped off, small droplets of blood appear, resembling dew.
Since the treatment of psoriasis and LP is significantly different, it is important to consult a doctor at the first manifestations, so as not to waste time and not aggravate the situation.
July 15, 2020
Author of the article: dermatologist Mak Vladimir Fedorovich
Is this disease contagious? What are the causes of the disease?
The mechanism of this disease is very complex, versatile and still not fully understood, although some of its stages are already known. This disease is not contagious. It is believed that there is a genetic predisposition to the disease. However, if one family member is sick, this does not mean that others will necessarily get lichen planus. Psoriasis can be triggered and complicated by various factors:
- physical injuries, chemical irritants,
- infection,
- stress,
- various medicines,
- alcohol,
- metabolic disorders (obesity, diabetes mellitus),
- other skin diseases, especially those causing itching.
How to understand whether we have lichen or psoriasis
To summarize all of the above, we can highlight several similar features of the two diseases:
- autoimmune nature;
- rash in the form of papules;
- itching;
- red papules;
- The flexures of the arms and legs are often affected.
The question arises of how to distinguish psoriasis from lichen. The diseases have several differences:
- psoriatic plaques peel off, scales can be seen on the surface, and with lichen planus the surface of the papules is smooth;
- psoriasis does not occur on mucous membranes, but LLP often affects the oral cavity and mucous surfaces of the genitals;
- plaques of psoriasis are larger than those that form with lichen;
- If lichen planus affects the scalp, cicatricial alopecia may occur.
Is phototherapy safe for treating lichen planus?
The Outpatient Comprehensive Lichen Squamosus Treatment Center at our GK Clinic has one of the most modern computerized equipment from Waldmann, designed for the effective and safe treatment of lichen planus and other skin diseases. Computerized equipment for phototherapy and assessment of skin type, determination of the minimum erythemal dose can reduce the possible harmful effects of ultraviolet radiation (phototoxic reactions and carcinogenic effects).
Modern ideas about psoriasis and methods of its treatment
The paper outlines the current views of psoriasis, a most common chronic skin disease. It details the treatments and the agents used in the therapy of the disease and compares the effectiveness of climatotherapy on the Black Sea shore, as well as on the Dead Sea shore in Israel. P
soriasis (scaly lichen) is one of the most common skin diseases; it is a chronic disease that lasts for years, accompanied by alternating relapses and remissions.
Epidemiology
According to statistics provided by various authors, about 2% of the world's population suffers from this disease (for example, in Denmark - 2.9, in Northern Europe (including England) - 2, USA - 1.4, China - 0.37%) .
Clinic
Psoriasis is characterized by the presence of a monomorphic rash in the form of nodules (papules) with a diameter of 1-3 mm to 2-3 cm or more, pink-red in color, covered with loosely sitting silvery-white scales. When papules are scraped, symptoms characteristic of psoriasis are revealed: “stearic spot”, “terminal film”, “blood dew”. The onset of the disease varies from patient to patient. More often, at the beginning of the disease, there are few rashes; they can persist for a long time in the same places, especially on the scalp and in the area of large joints, gradually progressing, usually under the influence of some provoking factors (trauma, poor diet, pregnancy or childbirth and etc.). After infectious diseases (flu, sore throat, etc.), severe nervous shock, drug intolerance, a profuse rash with many elements, usually small, swollen, located all over the skin, can immediately develop. As the disease develops, the number of elements increases, and their peripheral growth occurs, the papules merge and form plaques of various sizes and shapes. Characteristic of psoriasis is the Koebner phenomenon (a symptom of an isomorphic reaction), when psoriatic papules characteristic of the disease appear at the site of an injury or scratch. The favorite localization of psoriasis is the extensor surfaces of the extremities, especially in the area of the elbow and knee joints. The rash may affect the skin of the torso. The scalp is often affected. During psoriasis, progressive, stationary and regressive stages are distinguished. The progressive stage is characterized by the appearance on new areas of the skin of a large number of small, pinhead-sized, nodular rashes, there is a tendency towards peripheral growth of elements and the development of psoriatic papules.
Rice. Vulgar psoriasis
In the stationary stage, new elements do not appear. The existing papules on the skin stop increasing. The regressive stage of psoriasis is characterized by flattening of psoriatic plaques, decreased peeling and resorption of elements, which most often begins from the central part. In place of regressed rashes, as a rule, depigmented spots remain.
Classification of psoriasis
The following clinical types of psoriasis are distinguished: ordinary, exudative, arthropathic, psoriatic erythroderma and pustular psoriasis. Exudative psoriasis
(psoriasis exsudativa) differs from the clinical picture of ordinary psoriasis by significant exudation, as a result of which yellowish lamellar scales and crusts form on the surface of the papules.
When scale-crusts are removed from the surface of the papules, a weeping, bleeding surface is exposed. Pustular psoriasis
(psoriasis pustulosa) can manifest itself in a generalized or palmoplantar form. Generalized pustular psoriasis is severe, with fever, malaise, leukocytosis, and increased ESR. Small superficial pustules appear in paroxysms against the background of bright erythema, accompanied by burning and pain, located both in the area of plaques and on previously unchanged skin. Pustular psoriasis of the palms and soles is more common than the generalized form. The rashes, as a rule, are symmetrical and represent intraepidermal pustules against the background of severe hyperemia, infiltration and lichenification.
Rice. Exudative psoriasis
Arthropathic psoriasis
(psoriasis arthropathica) is characterized by the presence of typical skin rashes, accompanied by damage to joints, mainly small ones (hands and feet), less often large ones.
The range of clinical manifestations can vary from minor arthralgia, especially at the beginning, to a disabling condition. The distal joints are most often affected. At the onset of the disease, mono- or oligoarthritis is observed, usually asymmetrical; with a progressive course, generalized joint damage may develop. Swelling, pain, and limited joint mobility are noted as a result of infiltration and compaction of the periarticular tissues. In the further course of the process, dislocations, subluxations, and ankylosis may form, leading to deformation of the joints, and the patient’s disability often occurs. Psoriatic erythroderma
(erythrodermia psoriatica) is an acutely developing, generalized process, characterized at the peak of its development by the following symptoms: severe hyperemia, swelling, infiltration and lichenification, with a large number of scales on the surface. The patient's temperature rises, joint pain occurs, and general health worsens. Erythroderma can develop due to the gradual progression of the psoriatic process, the fusion of plaques, as well as under the influence of provoking factors, among which the most unfavorable are excessive insolation, an overdose of ultraviolet rays or their use (as well as irritating external agents) in a progressive stage. With psoriasis, nail lesions may be observed, manifested by pinpoint impressions on the surface of the nail plates (the “thimble” symptom), clouding or the appearance of longitudinal and transverse grooves. Sometimes the nail plates are thickened, deformed, and their surface is uneven. In other cases, nails crumble, break and are torn off.
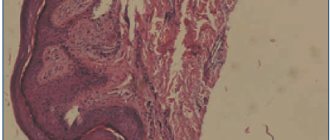
Histopathology
A pathognomonic sign of psoriasis is significant acanthosis with the presence of elongated epidermal outgrowths, somewhat thickened in their lower part. Above the apexes of the dermal papillae, the epidermis is sometimes thinned, parakeratosis is characteristic, and in older lesions there is hyperkeratosis. The granular layer is unevenly expressed and is absent under areas of parakeratosis. In the progressive stage, inter- and intracellular edema and exocytosis are noted in the stratum spinosum with the formation of focal accumulations of neutrophilic granulocytes, which, migrating into the stratum corneum or parakeratotic areas, form Munro microabscesses. Mitoses are often found in the basal and lower rows of the stratum spinosum. According to the lengthening of the epidermal outgrowths, the papillae of the dermis are elongated and expanded, sometimes flask-shaped, swollen, the vessels in them are tortuous, overflowing with blood. In the subpapillary layer there is a perivascular infiltrate of lymphocytes and neutrophilic granulocytes.
Etiology and pathogenesis
Psoriasis is a multifactorial disease. There are two types of psoriasis. Type I psoriasis is associated with the HLA antigen system (HLA Cw6, HLA B13, HLA B 17). This type of psoriasis affects 65% of patients; the onset of the disease occurs at a young age (18-25 years). Type II psoriasis is not associated with the HLA antigen system and occurs at an older age. Undoubtedly, changes in the immune system, caused either genetically or acquired under the influence of external and internal factors, play a large role in the pathogenesis of psoriasis. Provoking factors may include skin injuries, stress, the use of certain medications, alcohol abuse, infectious diseases (especially those caused by streptococcus, viral diseases), etc. Immune system disorders are detected both at the cellular and humoral level and consist of changes in the content of immunoglobulins of the main classes, circulating immune complexes, a pool of lymphocytes in peripheral blood, B and T populations and subpopulations of lymphocytes, killer cells, phagocytic activity of segmented leukocytes. It is believed that primary changes in psoriasis occur both at the level of cells of the dermal layer and the epidermis. Dysregulation in dermal cells causes excessive proliferation of the essentially normal epidermis. Hyperproliferation of keratinocytes leads to the secretion of cytokines and eicosanoids, which exacerbate skin inflammation. In epidermal lesions, antigen-presenting cells produce interleukin-1. It is likely that interleukin-1 is identical to epidermal T-lymphocyte activating factor (ETAF), which is produced by keratinocytes and activates thymic lymphocytes. Interleukin-1 determines the chemotaxis of T lymphocytes and, by stimulating their migration into the epidermis, may be responsible for the infiltration of the epidermis by these cells.
Rice. Psoriasis of the palms
Interleukins and interferons produced by T lymphocytes can themselves be mediators in the processes of hyperproliferation of keratinocytes, as well as mediators of inflammation and thus contribute to the maintenance of the vicious circle that determines the chronic nature of psoriasis.
Treatment
In accordance with the pathogenetic processes, therapy for psoriasis should be aimed at eliminating inflammation, suppressing the proliferation of epithelial cells, and normalizing their differentiation. To date, many different drugs and methods of treating psoriasis have been developed. Given the limited scope of this publication, the most effective of them are presented here. When prescribing treatment for patients with psoriasis, it is necessary to take into account the prevalence of skin lesions, stage of the disease, age, gender, the presence of concomitant diseases and contraindications to a particular treatment method or drug. Therapy for psoriasis should be comprehensive and combine the use of both drugs for local (external) and systemic therapy. External therapy.
The use of local drugs reduces inflammation, peeling and infiltration of the skin. These drugs include ointments and creams containing salicylic acid (2%), sulfur (2-10%), urea (10%), dithranol (0.25-3%), as well as glucocorticoid creams, ointments and lotions (solutions ). Lotions are commonly used to treat scalp lesions. In the progressive stage of the disease, salicylic ointment or anti-inflammatory hormonal ointments are usually prescribed. They start with the easiest ones - hydrocortisone, prednisolone. In case of repeated exacerbations or severe inflammation, it is necessary to use stronger fluoridated drugs (celestoderm, sinalar, vipsogal, belosalik and others). For example, when using Belosalik ointment containing b-methasone dipropionate and salicylic acid, 60-70% of patients experience complete regression of the rash within 14 days. When the lotion is prescribed for 21-28 days, a pronounced clinical effect is observed in more than 80% of patients. In recent years, non-halogenated glucocorticoid ointments (Advantan, Elokom) have begun to be used. Components containing fluorine and chlorine were removed from the composition of non-halogenated ointments, which significantly reduced the risk of local and systemic side effects. They can be used in the elderly and in early childhood. Creams and ointments containing dithranol (psorax, cignolin, cignoderm) have a pronounced antipsoriatic effect. Dithranol has antiproliferative and anti-inflammatory effects. The drug is prescribed in increasing concentrations using two methods: short-term (applied to the rash for 20-30 minutes) or long-term (applied once a day). The duration of common forms of the disease ranges from 2 to 8 weeks. Significant improvement and clinical recovery as a result of therapy with dithranol was noted in 70% of cases. Possible side effects of the drug include the development of local edema, itching, and erythema. Recently, a remedy has appeared whose action is based on a direct effect on the pathogenetic components of psoriasis. This is psorcutan ointment. Its chemical structure is based on calcipotriol, a synthetic analogue of the most active metabolite of vitamin D3. By interacting with keratinocyte receptors, it suppresses their excessive division, normalizes the processes of morphological differentiation, and has anti-inflammatory and immunocorrective properties. These properties of psorcutan determine good treatment results. To date, extensive clinical experience has already been accumulated in the use of psorcutan. According to the Center for Combating Psoriasis, which treated more than 200 patients with psorcutan, the effect, as a rule, is observed already on the 7-10th day from the start of therapy: peeling disappears, rashes turn pale, smooth out and flatten. By the end of the 8th week, there is a complete disappearance of rashes or a significant improvement in skin condition in the vast majority of patients. It is important that psorcutan, unlike glucocorticoid drugs, does not cause skin atrophy and gives a lasting effect after use. Remission of the disease sometimes lasts more than a year. It is good to combine psorcutan treatment with ultraviolet irradiation (PUVA or SFT). The pronounced clinical effect in the form of regression of rashes with psorcutan monotherapy is 43%, when combined with selective phototherapy - 86% and PUVA - 91%. With a long course of the disease, with frequent and constant exacerbations of psoriasis, it makes sense to periodically change ointments or alternate them, since the skin gets used to the medications and ointment used for a long time has less effect.
Systemic therapy
Aromatic retinoids.
Aromatic retinoids, which have been used for about 20 years in dermatological practice to treat a number of skin diseases, have taken a leading place in the treatment of patients with psoriasis.
The mechanism of action of aromatic retinoids in psoriasis is to inhibit the proliferation of epithelial cells, normalize the processes of keratinization and stabilize the membrane structures of cells, including liposomes. Developments in recent years have led to the introduction of a new aromatic synthetic analogue of retinoic acid - acetritin. Unlike its predecessor, etretinate, it has a number of significant advantages: it does not accumulate in the body and its half-life is 50 hours (versus 100 days). This allows you to avoid or quickly eliminate a number of side effects that occur during treatment with aromatic retinoids. Acetritin is the active ingredient of a drug called neotigazone. Neotigazon is used in a dosage of 20-25 mg per day. If necessary, the dosage of the drug can be increased to 50-75 mg per day. The course of treatment lasts 6-8 weeks. Treatment with neotigazon has a pronounced therapeutic effect in the treatment of psoriasis of the scalp, psoriatic arthritis and psoriatic lesions of the nail plates. Many years of experience in the use of aromatic retinoids at the Psoriasis Center in more than 3,000 patients has shown that the most effective is the combined use of retinoids with ultraviolet irradiation (PUVA or SFT) and local antipsoriatic drugs that affect proliferative processes in the skin. For comparison, the following figures can be given. Monotherapy with aromatic retinoids leads to clinical cure in 12% of patients, significant improvement in 41% and improvement in 47% of patients. Combination therapy produces clinical cure in 84% of cases, significant improvement in 12%, and improvement in 4% of cases. In cases where there are contraindications for the use of ultraviolet irradiation, a pronounced clinical effect (67%) is obtained by combining retinoids with psorcutan. Cyclosporin A
is a cyclic polypeptide that has an immunosuppressive effect.
The effect of cyclosporine is due to the suppression of the secretion of interleukins and other lymphokines by activated T-lymphocytes, which leads to a decrease in the activity of T-lymphocytes both in the dermal layer and in the epidermis of patients with psoriasis and indirectly affects the condition of blood vessels, hyperproliferation of the epidermis, as well as the activity of inflammatory cells. Along with this, cyclosporine suppresses the growth of keratinocytes. This effect may be due to inhibition of keratinocyte growth factor from mononuclear leukocytes in combination with a direct effect on keratinocyte growth. Cyclosporine is indicated for patients with severe forms of psoriasis when conventional therapy is ineffective or there are contraindications to other treatment methods. The drug is prescribed at the rate of 1.25 - 2.5 mg per 1 kg of body weight per day. If necessary, the dose can be increased to 5 mg per 1 kg of body weight per day. The duration of treatment is 4-8 weeks. Methotrexate.
It is a folic acid antagonist and cytostatic.
Due to the antifolic effect, the drug inhibits DNA synthesis and cell reproduction and, to a lesser extent, the synthesis of RNA and protein. Cells with active proliferation, in particular skin epithelial cells, are most sensitive to the drug. Methotrexate is prescribed in especially severe cases of refractory psoriasis (arthropathic, pustular psoriasis, erythroderma). Methods of treatment with methotrexate are different. Taking into account the data on the pharmacokinetics of the drug, cell proliferation in psoriasis, it is most advisable to prescribe it in three doses orally at 2.5-5 mg with a 12-hour interval every week or once in doses of 7.5-25 mg orally or 7.5-30 mg intramuscularly or intravenously once a week. It is recommended to start treatment with a small dose (5-10 mg once a week), gradually increasing it to an effective therapeutic dose with good tolerability and normal laboratory tests. The course is continued for about 4 weeks. Non-steroidal anti-inflammatory drugs.
For arthropathic psoriasis, as well as to reduce the severity of inflammation in exudative psoriasis and erythroderma, non-steroidal anti-inflammatory drugs are prescribed: indomethacin, diclofenac (0.025-0.05 g 3 times a day), naproxen (0.25-0.75 g 2 times per day).
Daily doses and duration of treatment depend on the severity of inflammatory changes, intensity of joint pain, and drug tolerance. The duration of treatment is usually 4-6 weeks. Photochemotherapy
(PUVA).
Combined use of long-wave ultraviolet rays (UV-A) with a wavelength of 360-365 nm and a photosensitizer (8-methoxypsoralen). In photochemotherapy, the main importance is attached to the interaction of a photosensitizer activated by long-wave ultraviolet rays with DNA, with the formation of mono- or bifunctional bonds, leading to inhibition of cell proliferation due to the suppression of the synthesis of nucleic acids and proteins. The effect of photochemotherapy can also be associated with an immunomodulatory effect with the normalization of cellular immunity, a direct effect on immunocompetent cells in the skin, and an effect on the biosynthesis and metabolism of prostaglandins. Photochemotherapy is carried out with an initial dose of UVA equal to 0.25-0.5 J/cm2 according to the method of irradiation 4 times a week with a gradual increase in the dose of UVA by 0.25-0.5 J/cm2. The course of treatment usually consists of 20-30 procedures. Selective phototherapy
(SPT).
Selective phototherapy uses mid-wave ultraviolet rays (UV-B) at a wavelength of 315-320 nm. Treatment begins with a dosage of UV-B rays equal to 0.05-0.1 J/cm2 according to the method of 4-6 single irradiations per week with a gradual increase in the UV-B dose by 0.1 J/cm2 for each subsequent procedure. The course of treatment usually includes 25-30 procedures. Climatotherapy.
Good results are obtained by climatotherapy (sanatorium-resort treatment) on the Black Sea coast or on the Dead Sea in Israel. The healing factors of the Dead Sea include UV radiation, air temperature, humidity, atmospheric pressure and the composition of salts in the Dead Sea water. The Dead Sea is located 395 m below the level of the World Ocean, and these additional layers of the atmosphere, as well as evaporation from the surface of the water, filter and trap harmful rays of the sun, creating an ideal ratio of long-wave (UVA 315 - 390 nm) and medium-wave (UVB 300 - 315 nm) UV rays. The average relative humidity is low and the air temperature is high, the number of sunny days per year reaches 330. The Dead Sea area has the highest barometric pressure (800 mm Hg) on Earth. The oxygen content in the air is 6-8% of molecules per 1 m higher than at Mediterranean Sea level. Dead Sea water contains large amounts of minerals and salts. The salt concentration is approximately 300 g of salt per 1 liter of water, while in the Mediterranean Sea it is approximately 35 g of salt per 1 liter of water. Treatment on the Dead Sea coast includes sunbathing, starting from 5 - 15 minutes 2 times a day with a constant increase in solar exposure by 10 minutes to a maximum of 6-8 hours daily, in combination with sea baths lasting from 10 to 60 minutes 2 - 3 times in a day. Depending on the condition of the skin, the time spent in the sun and sea water is adjusted. Natural oils (avocado, olive), indifferent creams and moisturizers, shampoos containing Dead Sea minerals, and tar are used as external therapy. Sometimes, in the first days of treatment, ointments containing sulfur, salicylic acid and tar are used. The recommended length of stay at the Dead Sea is 28 days. As our observations showed, upon completion of the course of treatment, complete cleansing of the skin was observed in 68% of patients, significant improvement in 22%, and improvement in 10% of patients. None of the patients worsened. Aeroheliothalassotherapy on the Black Sea coast, according to L.T. Shetsiruli et al. (1983), showed the following results: after a 21-30-day course, 23.3% of patients showed remission of the disease, 40.2% had a significant improvement, and 36.3% had an improvement. The presented results and comparative data indicate the high effectiveness of climatotherapy at the Dead Sea.
Literature:
1. V.V. Vladimirov. Diagnosis and treatment of skin diseases. Moscow. 1995. 2. S.I. Dovzhansky, S.R. Utz. Psoriasis. Saratov. 1992. 3. Skin and venereal diseases. Ed. Yu.K. Skripkina. Moscow. Medicine. volume 2, 1995. 4. L.V. Menshikov. The effectiveness of treatment of patients with psoriasis at the Dead Sea (Israel). On Sat. New in the diagnosis and treatment of sexually transmitted diseases and skin diseases. Moscow, 1997;73-4. 5. Roenigk H., Maibach N. Psoriasis. 2nd ed. 1990. 6. Weinstein G., Gottlieb A. Therapy of Moderate-to-Severe Psoriasis. 1993.