Symptoms of papillomatous nevus
Papillomatous nevus, unlike simple moles, has an irregular shape and protrudes above the skin. Depending on the pigmentation, it can match the color of the skin or have a brown, brown tint. Black nevi are very rare. Sometimes pigmented hair passes through the papillomatous nevus. Papillomatous nevi occur both single and multiple. Most often, nevi are localized on the head, neck, and face, but there may be cases where they are located in other places of the skin.
A characteristic feature of a papillomatous nevus is its slow but constant increase in size. From the beginning of development it is not noticeable, but as it grows it begins to cause discomfort to a person. Nevus on the head are often injured when combing hair. As a result, inflammation may occur.
Papillomatous nevus is a serious cosmetic defect; it causes inconvenience and psychological discomfort to its owner. In adolescents and people with a delicate mental structure, this situation can cause prolonged depression.
Why does a warty nevus appear?
Scientists have come to the conclusion that the formation of moles begins at the embryonic stage of development.
Factors that provoke their formation in humans are:
- imbalance of female sex hormones in a woman during pregnancy
- the presence of infectious pathologies during pregnancy
- the influence of unfavorable environmental factors on a woman’s body during pregnancy
- hereditary factors
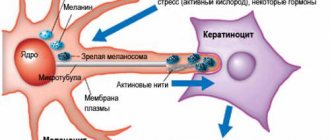
As a result of these reasons, the development process of melanoblasts, from which melanocytes are formed, is disrupted.
Melanocytes, concentrating in certain areas of the skin, turn into nevocytes.
Their difference from melanocytes is that they do not have processes that contribute to the spread of pigment.
Diagnosis of papillomatous nevus
For an accurate diagnosis, you need to consult an oncologist or dermatologist.
If a mole protrudes significantly beyond the skin, but does not cause discomfort, it should still be shown to a dermatologist. Accurate diagnosis of this type of skin formation is necessary in order to exclude melanoma and melanoma-dangerous nevi. Also, the type of tumor will help the doctor decide on treatment tactics. As a rule, a dermatologist will immediately distinguish a papillomatous nevus from an ordinary mole. Siascopic examination can be used for diagnosis. In difficult cases, a tumor biopsy, skin ultrasound and in-depth dermatoscopy are performed. In oncology, there are several types of nevi, depending on the size:
- small - up to 1.5 cm;
- medium - up to 10 cm;
- large - up to 20 cm;
- giant more than 20 cm.
A patient's risk of developing cancer directly depends on the size of the nevus.
Based on the place of their formation, nevi are divided as follows:
- epidermal - are an accumulation of melanocytes in the upper layers of the skin;
- intradermal - accumulation of melanocytes in the dermis;
- borderline - an accumulation of melanocytes between the upper layer of the skin and the dermis.
Features of care for verrucous nevus
If elements of a wart nevus are found on a patient’s body, doctors suggest removing it to remove the cosmetic defect.
If the patient for some reason does not want or cannot do this, then he must follow a number of rules that will help avoid the development of complications.
The basic rules are as follows:
- Eliminate factors that may cause overheating of moles. Prohibited: visiting saunas, baths, spa treatments.
- In the warm season, avoid being under the rays of the sun during the hours of its greatest activity: after 10 a.m. and before 4 p.m. Avoid visiting the solarium. It has been proven that protective agents cannot prevent the development of melanoma;
- Before taking hormonal medications, you should first consult with a specialist.
- Monitor the condition of the nevus elements and consult a doctor at the first symptoms of malignancy of moles.
You should pay attention to the following changes:
- accelerated nevus growth
- the appearance of unpleasant sensations that were not there before: pain, itching, burning, etc.
- change in the color of the neoplasm, it may become multi-colored
- appearance of peeling
- formation of cracks on the nevus
- hair loss
- asymmetrical growth, torn edges
- acquisition of granularity by a mole
- formation of outgrowths
- the appearance of discharge of various types
If at least one of the above symptoms appears, you should immediately consult a doctor.
If treatment turns out to be timely, then birthmarks will not pose a danger to a person in terms of malignancy.
And modern treatment methods will eliminate the presence of discomfort, both physical and cosmetic.
It is important to understand that self-medication can cause irreparable harm to health.
Removal of tumors should only take place in a medical facility and be carried out by a specialist.
Treatment of papillomatous nevus
Due to the fact that the nevus is constantly exposed to external factors, it can become damaged and then inflammation will begin, which can be easily recognized by soreness and redness. If during the diagnostic process doctors managed to completely exclude melanoma, dermatologists recommend removing the nevus with mandatory further histological examination of the formation.
Removal of papillomatous nevus can be carried out using a laser, cryodestruction, radio wave, electrocoagulation or surgical excision. Typically, all of the above operations are performed under local anesthesia.
Laser removal of warts
The use of lasers gives promising results. Various types of lasers have been used to treat moles, including: CO 2 lasers, dye laser. Landthalter et al. Dermatologists have successfully used argon laser in patients with localized papillary epidermal nevus. Also, very good results are achieved using the argon laser in most patients with superficial nevus, while satisfactory results have not been obtained in patients with papillary nevus.
Another method of laser treatment of warts is the removal of epidermal nevus with a pulsed Er: YAG laser operating at a wavelength of 2940 nm and having the properties of high absorption of water contained in the tissue, as well as CO 2 laser removal.
The pulse energy is aimed at ablation, and the area of thermal damage is small, which minimizes the possibility of scarring and guarantees a relatively rapid healing process. This type of laser can remove superficial changes with very good cosmetic results.
In the case of large papillary moles of the epidermis, the best method is CO2 laser treatment.
Uch. Michel et al have used the CO 2 laser in the treatment of papillary epidermal moles with good cosmetic results when the appropriate specifications are met. The small lesions have completely disappeared, leaving only a discolored scar. Relapses were observed with too gentle procedures.
Based on these results, scientists claim that CO 2 laser treatment is more effective than other lasers, but at the same time has a higher risk of scarring. Laser treatment is a relatively new, but very promising method of treating papillary nevi of the epidermis.
Sources
- Du Vivier A.: Atlas of Clinical Dermatology, 2002.
- Gur E, Zucker R: Complex facial nevi: a surgical algorithm, 2000.
- Rosen T: Keratoacanthomas arising within a linear epidermal nevus. J. Dermatol. 1982.
- Mikhalovsky R.: Dermatological syndromatology, 1984.
- Goldberg HS: Basal cell epitheliomas developing in a localized epidermal nevus. 1980.
- Ichikawa T. et al.: Squamous cell carcinoma arising in a verrucous epidermal nevus, Dermatology, 1996.
- Molin L, Sarhammar G: Perivulvar inflammatory linear verrucous epidermal nevus treated with CO2 laser, 1999.
- Michel JL et al: CO 2 laser dermabrasion in the treatment of linear papillary epidermal nevi, Dermatologica, 2001.
- Pavlacik M. et al.: Epidermal nevus syndrome - a two-symptomatic form, 1996.
- Zvulunov A. et al.: Calcipotriol for topical use for the treatment of inflammatory linear verrucous epidermal nevi: 1997.
- Pearson IC, Parland CC: Treatment of epidermal nevi with pulsed erbium laser, 2005.
- Boyce S, Alster TS: CO 2 laser treatment of epidermal nevi long-term success. 2002.
Surgical operations
Large papillomatous nevus undergoes surgical excision. The application of small cosmetic stitches after the removal operation guarantees minimal cosmetic defects. The possibility of relapse is excluded, since along with the nevus, the doctor also captures part of the healthy tissue when removing it. Giant nevi are also treated surgically. They are rare, but the risk of developing cancer in them is very high. Treatment of giant pigmented nevus is carried out in stages, with the involvement of plastic surgeons for further cosmetic operations.
Currently, there is no method that can prevent the appearance of a nevus. The only thing that can be avoided is the transformation of a nevus into melanoma. To do this, you just need to make sure that the nevus is not injured. Under no circumstances should you engage in self-extraction and self-diagnosis of nevi, as this may lead to undesirable consequences. Do not neglect your health, and if a large mole appears or damages an existing one, consult a doctor immediately.
- Gallery
- News
- Reviews
- Vacancies
- Licenses
- Insurance partners
- Controlling organizations
- Schedule for receiving citizens for personal requests
- What you need to know about coronavirus infection?
- Rules for patients
- Important! Visiting a clinic during self-isolation
- Online consultation with a doctor
- to corporative clients
- Documentation
Dysplastic nevus is one of the types of flat pigmented skin formations, which are more often called moles.
Patients, and many doctors, mistakenly believe that all flat pigmented formations are benign and do not pay attention to them. However, it is known that dysplastic nevi can transform into melanoma. The transformation process occurs gradually as lentiginous melanocytic dysplasia (LMD) develops from grade 1 to grade 3.
This type of formation deserves the closest attention among all types, since there is a very high risk of their malignancy with transition to the most malignant tumor - melanoma. The term dysplastic itself means that it is a nevus that is not similar in external and internal characteristics to typical moles. Dysplastic nevus, which occurs in 5%-9% of the white population, has recently attracted the attention of researchers, as it may be a precursor to superficial spreading melanoma: it is found in almost all patients with hereditary melanoma and in 30–50% of patients with sporadic melanoma . A dysplastic nevus can occur on intact skin or be a component of a complex noncellular nevus.
Clinically, dysplastic nevus is similar to borderline nevus, but there are also differences. Thus, a dysplastic nevus is an irregularly shaped spot, while a borderline nevus has a regular shape - round or oval. The color of a dysplastic nevus is often heterogeneous, with areas of dark pigment, while a borderline nevus is characterized by a uniform color, the color of both nevi varies from light brown to dark brown. Often, a pinpoint formation resembling a target is noted in the center of a dysplastic nevus. When a dysplastic and mixed nevus is combined, there is a picture of a “fried egg” with a raised yolk in the center.
In our observations, dysplastic nevi were found in 5% - 10% of patients who consulted a surgeon or oncologist for various diseases. In some, the nevi were single - from 3 to 10 formations, in others - multiple - from 50 to 100 or more. Observing patients with multiple dysplastic nevi, we identified 2 types of these formations.
In the first type - there were fewer of these patients - dysplastic nevi appeared in childhood and adolescence, were often hereditary, but these patients did not report melanoma in relatives. Carriers of nevi were, as a rule, white-skinned, poorly tanned, with blond or red hair and light eyes. Dysplastic nevi of this type were large - 0.5 - 1.0 cm in diameter, located on open and closed areas of the body (buttocks, lower abdomen), and were often combined with papillomatous nevi. The color of nevi in the same patient could vary from pink to dark brown, sometimes a variegated color was observed: dark areas on a pink or light brown background. This pattern of nevi has been described as “dysplastic nevus syndrome.” After puberty, new nevi did not appear in this group of patients. This fact can be attributed to the fact that white-skinned people limited their exposure to the sun, as they quickly burned, and were also informed about the possible appearance of new “moles” as a result of exposure to ultraviolet radiation.
In the second type, dysplastic nevi were rare in adolescence; most nevi appeared in adulthood and were associated with frequent and prolonged exposure to the sun while vacationing in southern latitudes. Dysplastic nevi of this type were small - from 0.1 to 0.4 cm in diameter, regular rounded in shape, uniform in color, combined with multiple freckles in young patients and pigment spots of the “Dubreuil’s melanosis” type in older patients. In white-skinned patients with skin phototype 1 - 2, the nevi were light brown, in others they were brown or dark brown. The density of nevi was higher on sun-exposed areas of the body: the face, forearms, outer surface of the shoulders, upper half of the back and chest wall (like a “wide neckline”). All this indicates some similarity between dysplastic nevi of the second type and Dubreuil’s melanosis, which is a proliferation of melanocytes in the basal layer of the epidermis in individuals with skin phototype 1 - 2 under the influence of repeated sunburn.
According to our observations, the most important sign of progression of dysplastic nevus is:
- The appearance of pigment formation on unchanged skin and its further growth over several months or years in persons over 18 years of age , i.e. in adulthood.
- Changes in the last 3-5 years of a long-existing nevus may indicate the progression of a dysplastic nevus, which is combined with a borderline or mixed nevus.
- An important sign of a progressive dysplastic nevus is a very dark color (almost black), or uneven coloration of the formation with areas of dark brown or black.
- The irregular shape of the nevus may be little noticeable with a small size of the progressive dysplastic nevus , at the same time it can also be observed in a long-existing noncellular nevus - borderline or mixed.
Excision of dysplastic nevus
Excision of the nevus (excisional biopsy) should be performed under local anesthesia, 0.4–1.0 cm from the visible boundaries, with subcutaneous tissue. Histological examination of a removed nevus should be carried out by a pathologist with experience in the study of melanocytic formations. Progressive dysplastic nevi require excision for prevention purposes, as well as early diagnosis of cutaneous melanoma . When melanoma is detected, the question of the need for reoperation - excision of the postoperative scar - is decided depending on the thickness of the tumor, determined by histological examination. According to foreign authors, as well as WHO recommendations, an adequate deviation from the boundaries of the formation for in-situ melanoma is 0.2 - 0.5 cm, for invasive melanoma with a thickness of less than 1.5 mm - 1.0 cm.
During removals carried out in the department of surgery from June 2009 to April 2014, of all removed pigmented formations, the clinical diagnosis of “dysplastic nevus” was confirmed morphologically in 76% of cases, i.e. Histological examination of these formations revealed structures of lentiginous melanocytic dysplasia (LMD). In 2.4% of cases, melanoma was detected that developed against the background of LMD ; in other cases, other types of nevi were confirmed (intradermal, mixed nevus, nevus of the sebaceous glands). In our clinical cases, patients with diagnosed melanoma did not require reoperation.
Foreign authors recommend removing dysplastic nevi 0.6 cm or more; according to our research, smaller nevi - 0.4 - 0.5 cm in diameter - can also be removed. In our practice, melanoma in one case measured 0.5 x 0.4 cm, in another - 0.5 cm.
Photos 1 and 2 show dysplastic nevi with signs of progression.
Photo 1 shows a nevus of the gluteal region measuring 0.5 x 0.4 cm in a 29-year-old patient with skin phototype 1. The nevus, according to the patient, appeared 7 months ago in the form of a punctate formation, which gradually increased (a sign of progression) . No other pigmented nevi or freckles were found on the body. Histological examination: lentiginous pigmented nevus with severe (grade 3) melanocytic lentiginous dysplasia.
Photo 2 shows a nevus of the chest wall in a 27-year-old patient , 0.3 cm in diameter, round in shape, which darkened after staying in the south (a sign of progression) . Histological examination - mixed dysplastic pigmented nevus with severe (grade 3) melanocytic lentiginous dysplasia.
If the patient refuses surgery or in the absence of obvious signs of progression of the dysplastic nevus, the nevus should be re-examined by a doctor after 6 months. If there are changes in the nevus over the past period, surgery is recommended; if there are no changes, further observation after 6 months.
Patients with dysplastic nevi need:
- avoid prolonged exposure to direct sunlight,
- protect the skin with clothing,
- apply sunscreen.
The material was prepared based on the article: “Tactics for managing a patient with a dysplastic nevus” - O.A. Romanova, N.G. Artemyeva, E.A. Yagubova, I.M. Rudakova, V.N. Marycheva, A.A. Veshchevaylov . Clinical dermatology and venereology No. 2, 2015.
Services and prices
Histological examination of skin biopsy material
1,650 rub.
Appointment with a dermatovenerologist, therapeutic and diagnostic, primary, outpatient
2,000 rub.
Appointment with a dermatovenerologist, therapeutic and diagnostic, repeat, outpatient
1,800 rub.
Appointment with an oncologist, treatment and diagnostic, primary, outpatient
2,000 rub.
Appointment with an oncologist, therapeutic and diagnostic, repeated, outpatient
1,800 rub.
Appointment with a surgeon LD, PERV, AMB
2,000 rub.
Appointment with a surgeon, candidate of medical sciences, primary, outpatient
2,500 rub.
Removal of benign formations with a diameter of up to 5 mm using the molecular resonance surgical device VESALIUS LX 80 (with anesthesia and bandage)
2,500 rub.
Removal of a benign tumor with a diameter of more than 5 mm using a molecular resonance surgical device VESALIUS LX 80 (with anesthesia and bandage)
3,100 rub.
Isaeva Galina Ivanovna Oncologist Work experience: 19 years
Romanova Olga Aleksandrovna Oncologist (mammologist) Work experience: 62 years
Artemyeva Nadezhda Georgievna Head of department, surgeon, phlebologist Doctor of the highest category Work experience: 43 years
Bezlepko Marina Gennadievna Oncologist Work experience: 13 years
Make an appointment
Is HPV the cause of nevus?
Need advice from an experienced doctor?
Get a doctor's consultation online. Ask your question right now.
Ask a free question
Intradermal papillomatous nevi resemble papillomas in appearance. The appearance of the melanocytic element is not associated with papillomavirus. Two similar skin growths differ in etiology and structure. Papillomatosis (code D 23 according to ICD-10) is a chronic infection caused by HPV activity. The pathology affects children and adults. The main route of transmission of the virus is through household contact, sexual contact, and intrapartum.
Melanocytic papillomatous intradermal warty nevus is formed by melanocytes. The reasons for its appearance on the human body are not fully understood. There are several theories of origin:
- According to the first theory, education is transmitted along the family line. Confirms the fact of similar localization in parents and children.
- The second theory is based on excess melanin secretion. Melanocytes accumulate under the skin in one place and begin to intensively secrete coloring pigments. Active production of melanin occurs under the influence of ultraviolet radiation.
- According to the third theory, the formation of an intradermal growth occurs in the prenatal period. The appearance of bumpy formations is provoked by the mother’s addictions, inflammatory diseases, and contact with harmful substances.
- The fourth theory associates the occurrence of growths with hormonal disorders. Melanocyte-stimulating hormone of the pituitary gland activates melanocytes, which begin to synthesize melanin.