1.What is idiopathic urticaria?
Hives
is a skin reaction that most people have experienced at least once in their lives.
Most often, itching and skin rashes have specific causes (which can range from foods eaten and plant odors to liver disease, parasites or exposure to cold). Atypical diseases of unclear, purely individual origin are considered idiopathic. Thus, idiopathic urticaria
is itchy skin that has no specific cause.
Idiopathic urticaria can develop in a person of any age and social status, in any climate zone, and is one of the most common diseases. 25% of cases of causeless skin allergies become chronic.
There is no consensus on the causes of idiopathic urticaria, but most doctors are inclined to the hypothesis that antibodies are not working correctly, which for some reason begin to attack their own body and thereby disrupt its immune status.
A must read! Help with treatment and hospitalization!
Principles of treatment of urticaria and angioedema
Urticaria and angioedema (angioedema) (AO) are widespread skin diseases that have a significant negative impact on the patient’s quality of life. They are usually easy to diagnose, but not always easy to treat due to varying severity, frequent resistance to antihistamines, and the presence of other diseases in the patient, which are the primary cause of the skin process. In addition, not all specialists are familiar with the leading guideline documents; many of them do not know the specifics of treatment of acute urticaria ((OK), lasting less than 6 weeks) and chronic urticaria ((CU), lasting more than 6 weeks) and are not always able to choose the right one therapeutic and/or diagnostic tactics for a particular patient.
The purpose of this review is to briefly describe the main methods of treatment of various types of urticaria in adult patients and older children and the drugs used, based on existing scientific evidence.
To optimize pharmacotherapy and select further treatment tactics, it is important to determine the type/form of urticaria (for example, physical/vibrational), its duration (acute, episodic or chronic). The features of such diagnostics are described in other publications [1, 22].
The goal of treatment is to achieve control of the disease and the associated improvement in the quality of life of patients, the ability to work or study, and also to minimize side effects mediated by the use of drugs. This is especially important when treating long-term forms of chronic urticaria. To assess disease control, you can take into account the severity of itching, AO, the size of blisters, their number and frequency of occurrence, night awakenings and the duration of remission of the disease.
Treatment aimed at causative and precipitating factors
First of all, the underlying disease (if identified) that causes urticaria is treated. It is necessary to do everything possible (carry out all the necessary diagnostic tests) to identify the cause and provoking factors of urticaria in case of its chronic course. After determining the latter, it is necessary to exclude contact with them, for example, do not take Aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) if you are sensitive to them (many NSAIDs cause exacerbation of CU in 20-30% of patients, even with another cause) or angiotensin-converting enzyme inhibitors (ACEIs). ) with recurrent AO.
Elimination of provoking factors
Exclusion of provoking factors is an effective type of treatment and prevention if these factors are known or suspected (food product, drugs, physical stimulus, etc.).
Many experts recommend that all patients with urticaria avoid taking pseudoallergens, Aspirin and other NSAIDs, and ACE inhibitors as possible nonspecific triggers [2], although reliable evidence for this statement is lacking.
Patients with acute allergic urticaria should avoid contact with identified causally significant allergens, and with physical allergens, avoid exposure to a causative physical stimulus depending on the type of urticaria: sunlight, mechanical irritation, skin compression, vibration, water, cold, heat, overheating, physical loads.
In many cases, alcohol, stress and overheating increase the manifestations of CU (Table 1).
Diet
In patients with allergic IgE-related urticaria, it is important to exclude causative foods from the diet. On the other hand, allergies to food and food additives in chronic chronic disease are extremely rare, despite widespread misconception. Data on the need to prescribe a diet with a limitation of food additives (dyes, preservatives, flavor enhancers, aromas, etc.) [5–7] and natural salicylates (so-called pseudoallergens) to patients with Aspirin-sensitive CU are contradictory. In a prospective, open-label study that included 64 patients, 73% of patients with CU showed an improvement in the skin process when following a strict diet with the exclusion of pseudoallergens for 2 weeks, but confirmation of the reaction after a provocative test with individual pseudoallergens was recorded in only 19% of them [ 8].
Treatment of physical urticaria. Tolerance induction
In motivated patients with cold, solar, cholinergic and generalized thermal urticaria, desensitization (induction of tolerance) is possible. The procedure involves repeated exposure of the patient's skin to a stimulus, such as cold or heat, until it becomes refractory (i.e., does not respond to provocation) [9–11]. Exposure to the stimulus must be regular and of sufficient intensity, otherwise tolerance will disappear within a few days [1].
Treatment of autoimmune urticaria
It is believed that in about 50% of patients, CU has an autoimmune form, which is confirmed using laboratory methods and intradermal autologous serum test (IAT).
Currently, protocols are being developed to carry out desensitization in patients with autoimmune CC using injections of autologous serum or whole blood [12, 13]. The goal of this treatment is to induce tolerance to circulating histamine-releasing factors. In a Turkish study published in July 2011, the authors used injections of autologous serum, autologous plasma, and placebo in three parallel subgroups of patients with both TAC-positive (TAC+) and TAC-negative (TAC-) responses [14]. The effectiveness of treatment with autologous serum and plasma was almost equal to that in the placebo group (the difference was not statistically significant), despite this, in patients with TAC+ and TAC– there was a decrease in urticaria activity and an increase in quality of life indicators. Taking into account these data, the effectiveness of autohemotherapy in patients with CU needs further study.
Treatment of concomitant infections
The need for treatment of chronic foci of infection in urticaria, in particular Helicobacter pylori, is still under debate. There are studies (including Russian ones) confirming that eradication of H. pylori can lead to a significant improvement in the course of urticaria [15, 16], while in others, antibacterial treatment did not have any significant effect on the symptoms of CU [ 17, 18].
The role of this microorganism in the pathogenesis of CC and AO remains controversial. The frequency of infection in the general population is very high [19], so H. pylori is detected in 40–50% of patients with CU. Some experts recommend, even in the absence of scientific evidence of effectiveness, prescribing antibacterial treatment to patients with CU both for the eradication of H. pylori and for other subclinical infectious diseases (streptococcal, staphylococcal, yersiniosis, etc.), although, according to research data, such an approach does not always lead to improvement in urticaria symptoms.
Further randomized clinical trials (RCTs) are required to examine the effects of antibiotic therapy and H. pylori eradication on urticaria.
Treatment of acute urticaria
Acute spontaneous urticaria can be allergic or non-allergic. But the treatment in both cases is practically the same. In more than 90% of cases, the acute form of the disease resolves spontaneously [1].
Indications for hospitalization:
- severe forms of OK and AO in the larynx with a risk of asphyxia;
- all cases of anaphylactic reaction accompanied by urticaria;
- severe forms of exacerbation of OK, CC and AO, resistant to outpatient treatment.
Initial treatment measures include addressing the cause: stopping the use of the causative drug or food product, removing the insect sting, and prescribing antibiotics for a bacterial infection. Subsequently, symptomatic pharmacotherapy is carried out.
Despite long-term and widespread use, only a few RCTs have been published on the use of second-generation histamine H1 receptor blockers (H1-HBs) (first-choice drugs) and short courses of systemic glucocorticosteroids ((GCS), second-choice drugs) for CC [1] .
Initial symptomatic therapy includes the administration of non-sedating N1-BG with the possibility of increasing the daily dose in adult patients 4 times higher than that indicated in the instructions for the drug (possible side effects must be taken into account). In some cases, especially with limited urticaria, topical treatment is used - antipruritic and cooling lotions (for example, 1% and 2% water-based menthol) [1].
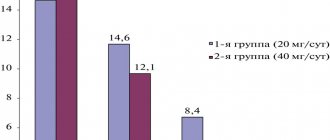
Second-line drugs include corticosteroids prescribed orally at 50 mg/day in a short course for 3 days [20] or 20 mg 2 times a day for 4 days [21].
In severe cases of urticaria (for example, when combined with AO or with a high risk of developing anaphylaxis), some experts recommend intravenous administration of corticosteroids (30–100 mg of prednisolone or 4–16 mg of dexamethasone or more) and sedative H1-BG, incl. and again [22].
In severe, progressive cases with the development of anaphylaxis and shock, therapy should be carried out in conjunction with parenteral administration of epinephrine.
Most cases of OC respond well to treatment with N1-GD and corticosteroids. However, symptoms may reappear after a few hours (in some patients, symptoms persist for up to 2 weeks or more). In these cases, patients should receive non-sedating second-generation N1-GDs in adequate doses (up to a 4-fold increase in adult patients) for the required time; such patients should be advised to have corticosteroids in tablets (for example, prednisolone) at home in case symptoms worsen.
The use of topical N1-BG should be avoided due to its limited effect and possible sensitizing potential.
In most cases, it is impossible to predict whether acute urticaria will become chronic. It is also unclear whether such a transition is influenced by the administration of adequate treatment or not.
Treatment of chronic urticaria
Unfortunately, the disease that causes the onset of CC is rarely detected, but if this can be done, then its treatment is carried out first. When the underlying disease is cured, there is a high probability of complete disappearance of urticaria symptoms. To a lesser extent, this applies to autoimmune urticaria associated with other autoimmune diseases, since, for example, even with complete control of autoimmune thyroiditis associated with hypothyroidism and autoimmune urticaria, an improvement in the course of the skin process is not always observed.
Key treatment features:
- treatment of the identified cause of urticaria (if possible);
- cessation/reduction of contact with provoking factors;
- explaining to the patient the features of the course, diagnosis and treatment of the disease (orally and in the form of notes);
- approach to relieve symptoms;
- trial administration of second generation N1-BG; increase the daily dose if necessary;
- use of second- and third-line drugs in patients with severe and treatment-resistant disease, including immunosuppressive and immunomodulatory drugs.
It is important to inform the patient with CU that:
- CC does not lead to progressive or irreversible tissue damage in all cases in the absence of an underlying disease that serves as its cause;
- the disease often stops spontaneously (approximately 50% of cases);
- food and allergies are almost never the cause of CC, so there is no need for extensive allergological examinations;
- It is necessary to have an first aid kit (especially for patients with recurrent laryngeal edema). The first aid kit should contain adrenaline/epinephrine (preferably in the form of an autoinjector), corticosteroids and antihistamines for parenteral administration, syringes and needles.
Another important direction of therapy is the use of drugs for symptomatic treatment in order to reduce the severity of skin rashes/itching/AO and prevent their reappearance.
Cooling lotions (eg, 1% water-based menthol cream, calamine lotion, and 10% crotamiton lotion) can be used as a topical treatment, especially in areas of severe itching. It must be borne in mind that alcohol-containing lotions, when applied to areas of damaged or eczematous skin, can exacerbate the exacerbation of the disease. Antihistamine creams and gels (eg, dimethindene) are widely used, but their pharmacological effectiveness is limited by poor skin absorption. Topical corticosteroids are practically not used in routine clinical practice for the treatment of chronic urticaria, but some studies have shown that when they are regularly applied to local areas of the skin, the severity of the urticarial response to pressure is reduced. This may be due to a decrease in the number of mast cells in these locations [23, 24].
According to the recommendations of the World Allergy Organization (WAO), in all cases of urticaria, treatment should begin with non-sedating second-generation antihistamines (drugs of first choice). Only if they are unavailable or ineffective in maximum doses, the use of sedative H1-BG is possible [25], which is limited by frequent side effects, in particular sedation and anticholinergic. In most patients, the use of second-generation antihistamines helps control the disease [26], however, adding first-generation H1-GD at night is logical and is allowed if the patient is bothered by severe night itching and associated insomnia.
Subsequently, depending on the response, treatment in adult patients is carried out according to the algorithm shown in Fig. The cost, safety and effectiveness of treatment are discussed in Table. 2.
It is important to remember that some patients with CU may not respond to standard doses of second-generation antihistamines. In this case, it is possible to increase the daily dose of a drug from this group by 2–4 times from that recommended in the manufacturer’s instructions. Both clinical experience and research data confirm that this approach (increasing the dose of non-sedating N1-GD) is associated with greater treatment efficacy and disease control in many (but not all) patients [29, 30].
If there is no effect from increasing the dose of H1-BG, you can add antileukotriene drugs or replace H1-BG with another one. If urticaria is ineffective or severe, alternative therapy with second or third line drugs, such as cyclosporine, a combination of H1- and H2-BG, dapsone or omalizumab, should be considered [25]. It is recommended to refrain from prescribing such treatment for up to 1–4 weeks, since the effect of taking antihistamines may be delayed [25].
The effectiveness of drugs may vary for each patient. It should also be taken into account that the drugs do not maintain a long-term effect after they are discontinued, therefore, for persistent urticaria, maintenance therapy is necessary. With long-term treatment, the development of tachyphylaxis is usually not observed, and in many patients with chronic idiopathic or autoimmune urticaria, symptomatic therapy leads to a significant positive response and control of the disease.
Further observation
In many cases, long-term use of drugs is necessary until remission of the disease occurs. For most patients with CU, 3–6 months of regular therapy is recommended [25]. In patients with a long history of urticaria and AO, treatment is carried out for 6–12 months with gradual withdrawal for several weeks. It was shown that patients with CU who took N1-BG continuously suffered from a less pronounced decrease in quality of life compared to those who used drugs occasionally [32].
Every 3–6 months or more often, it is necessary to examine and interview the patient to identify new symptoms (signs of autoimmune pathology, etc.), as well as to assess the severity of urticaria (it may change over time) and adjust therapy [25].
The average duration of CU is 3–5 years, although approximately half of patients experience spontaneous remission 0.5–1 year after onset. In approximately 40% of patients, CU that has existed for more than 6 months will recur over the next 10 years, and in 20% even over 20 years [31].
The goal of treatment for chronic disease is to minimize the manifestations of the disease against the background of optimally selected therapy until remission occurs.
Conclusion
Urticaria/AO is a heterogeneous group of diseases characterized by a variety of clinical manifestations and different mechanisms of development. Therefore, it is logical that a stepwise approach should be used to treat it, based on the form of urticaria, severity, pathogenesis and course characteristics.
As already mentioned, the key principle of therapy for both OC and CC in adult patients (and sometimes in children), which, unfortunately, is unknown to many Russian doctors, is the prescription of second generation antihistamines (drugs of choice) in a standard dose, and when their ineffectiveness - increase the daily dose up to 4 times from that specified in the instructions. This approach is approved and recommended by leading international and national communities and specialists, it is based on increasing the effect of H1-GD while maintaining relative safety (sedation, impaired cognitive and psychomotor functions and other side effects are usually absent even at high doses) compared to prescription GKS. It is important to emphasize here that from a legal point of view, the doctor does not have the right to deviate from the instructions for the use of a particular drug. To date, in all instructions for second generation antihistamines approved in Russia, there are no recommendations for increasing the dose. In addition, you should always weigh the possible benefits and risks of any type of treatment.
It must be remembered that antihistamines are indicated for almost all patients with urticaria, with the exception of some patients with isolated AO, in particular with hereditary AO. In addition, unless specifically indicated, it is advisable to avoid prescribing antihistamines and other systemic drugs in the first trimester of pregnancy, despite the fact that studies have not shown a teratogenic effect. The addition of leukotriene receptor blockers (montelukast, zafirlukast) to antihistamine therapy in adult patients may provide an additional effect when exacerbation of urticaria is associated with the intake of food pseudoallergens, aspirin, or the presence of functional autoantibodies.
Currently, additional research is required on existing drugs for the treatment of urticaria, especially urticaria, and the search for new highly effective drugs. It should be taken into account that the use of most second- and third-line drugs, in particular cyclosporine and omalizumab, is associated with high costs and/or a significant risk of severe side effects.
Literature
- Kolhir P.V. Urticaria and angioedema. M.: Practical Medicine, 2012.
- Wong JT, Nagy CS, Krinzman SJ et al. Rapid oral challenge-desensitization for patients with aspirin-related urticaria-angioedema // J. Allergy Clin. Immunol. 2000; 105(5):997-10-01.
- Zuberbier T., Pfrommer C., Specht K. et al. Aromatic components of food as novel identifying factors of pseudoallergic reactions in chronic urticaria // J. Allergy Clin. Immunol. 2002; 109: 343–348.
- O'Donnell BF, Francis DM, Swana GT et al. Thyroid autoimmunity in chronic urticaria // Br. J. Dermatol. 2005; 153:333–335.
- Young E. Prevalence of intolerance to food additives // Environ. Toxicol. Pharmacol. 1997; 4: 111–114.
- Zuberbeir T., Pfrommer C., Specht K. et al. Aromatic components of food as novel identifying factors of pseudoallergic reactions in chronic urticaria // J. Allergy Clin. Immunol. 2002; 109: 343–348.
- Guerra L., Rogkakou A., Massacane P. et al. Role of contact sensitization in chronic urticaria // J. Am. Acad. Dermatol. 2007; 56:88–90.
- Zuberbier T., Chantraine-Hess S., Harmann K., Czarnetski BM Pseudoallergen-free diet in the treatment of chronic urticaria. A prospective study // Acta Derm. Venereol. (Stockh.) 1995; 75:484–487.
- Champion RH A practical approach to the urticarial syndromes — a dermatologist's view // Clin. Exp. Allergy 1990; 20: 221–224.
- Cantani A. Pediatric Allergy, Asthma and Immunology. Berlin: Springer, 2008.
- Wanderer AA The spectrum of cold urticaria // Immunol. Allergy Clin. N. Am. 1995; 15: 701–723.
- Staubach P., Onnen K., Vonend A. et al. Autologous whole blood injections to patients with chronic urticaria and a positive autologous serum skin test: a placebo-controlled trial // Dermatology. 2006; 212: 156–159.
- Xiu MG, Wang DF Observation on therapeutic effect of acupoint injection desensitization with autoblood on chronic urticaria // Zhongguo. Zhen. Jiu. 2011; 31 (7): 610–612.
- Emek Kocaturk, Selin Aktas, Zafer Turkoglu et al. Autologous whole blood and autologous serum injections are equally effective as placebo injections in reducing disease activity in patients with chronic spontaneous urticaria: a placebo controlled, randomized, single-blind study // J. Dermatolog. Treat. 2011, Jul 31.
- Wedi B., Wagner S., Werfel T. et al. Prevalence of helicobacter pylori-associated gastritis in chronic urticaria // Int. Arch. Allergy Immunol. 1998; 116:288–294.
- DiCampli C., Gasbarrini A., Nucera E. et al. Beneficial effects of helicobacter pylori eradication on chronic idiopathic urticaria // Digest. Dis. Sci. 1998; 43:1226–1229.
- Schnyder B., Helbing A., Pichler WJ Chronic idiopathic urticaria: natural course and association with helicobacter pylori infection // Int. Arch. Allergy Immunol. 1999; 119: 60–63.
- Valsecchi R., Pigatto P. Chronic urticaria and Helicobacter pylori // Acta Derm. Venereol. 1998; 78:440–442.
- Becker H., Meyer M., Paul E. Remission ratio of chronic urticaria: “Spontaneous” healing as a result of eradication of helicobacter pylori? // Hautarzt. 1998; 49:907–911.
- Zuberbier T., Iflander J., Semmler C., Henz BM Acute urticaria: clinical aspects and therapeutic responsiveness // Acta Derm. Venereol. 1996; 76:295–297.
- Pollack CV Jr., Romano TJ Outpatient management of acute urticaria: the role of prednisone // Ann. Emerg. Med. 1995; 26:547–551.
- Zuberbier T., Grattan C., Maurer M. Urticaria and Angioedema. London: Springer, 2010.
- Barlow RJ, Macdonald DM, Kobza Black A. et al. The effects of topical corticosteroids on delayed pressure urticaria // Arch. Dermatol. Res. 1995; 287:285–288.
- Vena GA, Cassano N, D'Argento V et al. Clobetasol propionate 0.05% in a novel foam formulation is safe and effective in the short-term treatment of patients with delayed pressure urticaria: a randomized double-blind, placebo-controlled trial // Br. J. Dermatol. 2006; 154:353–356.
- Zuberbier T., Asero R., Bindslev-Jensen C. et al. EAACI/GA2LEN/EDF/WAO guideline: management of urticaria // Allergy. 2009; 64:1427–1443.
- Simons FER, Sussman GL, Simons KJ Effect of the H2-antagonist cimetidine on the pharmacokinetics and pharmacodynamics of the H1-antagonists hydroxyzine and cetirizine in patients with chronic urticaria // J. Allergy Clin. Immunol. 1995; 95:685–693.
- Powell RJ, Du Toit GL et al. BSACI guidelines for the management of chronic urticaria and angio-oedema // Clin. Exp. Allergy. 2007; 37: 645–650.
- Grattan CE, Humphreys F. British Association of Dermatologists Therapy Guidelines and Audit Subcommittee. Guidelines for evaluation and management of urticaria in adults and children // Br. J. Dermatol. 2007; 157(6):1116–1123.
- Staevska M., Popov T., Kralimarkova T. et al. The effectiveness of levocetirizine and desloratadine in up to 4 times conventional doses in difficult-to-treat urticaria // J. Allergy Clin. Immunol. 2010; 125:676–682.
- Dubertret L., Zalupca L., Cristodoulo T. et al. Once-daily rupatadine improves the symptoms of chronic idiopathic urticaria: a randomized, double-blind, placebo-controlled study // Eur. J. Dermatol. 2007; 17: 223–228.
- Volcheck GW Clinical Allergy: Diagnosis and Management, Mayo Foundation for Medical Education and Research. Abington: Humana Press, 2009.
- Grob J., Auquier P., Dreyfus I., Ortonne J. How to prescribe antihistamines for chronic idiopathic urticaria: desloratadine daily vs PRN and quality of life // Allergy. 2009; 64:605–612.
P. V. Kolkhir, Candidate of Medical Sciences
Research Center GBOU VPO First Moscow State Medical University named after. I. M. Sechenova Ministry of Health and Social Development of Russia, Moscow
Contact information about the author for correspondence
2.Symptoms of urticaria
Usually urticaria appears quite clearly. These are, first of all, skin disorders:
- itching and swelling of the skin;
- watery blisters;
- small purple rashes.
In severe cases, when large areas of skin are affected, an exacerbation may be accompanied by general malaise, sleep disturbances, headaches, chills, and neurotic disorders
caused by itchy skin.
Most often, idiopathic urticaria differs from other skin allergies by prolonged exacerbations, which can last up to one and a half months
. However, starting with small spots and blisters, urticaria lesions can merge with each other, forming larger zones.
Severe skin itching, in addition to purely cosmetic problems, is the main, very unpleasant and unsafe symptom of this disease. Constant daytime irritation causes serious psycho-emotional trauma, sometimes forcing the patient to take sedatives. Involuntary scratching during sleep is no less dangerous, since it carries the risk of infection of the resulting wounds and scratches. When the blisters are injured, a clear liquid is usually released, and then a dry crust forms, which also itches.
Visit our Dermatology page
Celery for hives
Celery contains many minerals and vitamins, so this plant is used as a traditional medicine. A number of numerous properties include: antiallergic, restorative and soothing.
In addition, its benefit lies in the ability to remove toxic substances from the body, while restoring the functioning of the intestinal tract. Eating celery is prohibited in case of acute inflammatory processes in the gastrointestinal tract, pancreatitis and kidney stones.
During pregnancy, it is recommended to reduce the consumption of celery.
There are several options for preparing traditional medicine from this plant:
NOTE!
To quickly get rid of blackheads, acne and pimples, as well as to rejuvenate your facial skin, we recommend that you familiarize yourself with this effective remedy .
Find out more...
- Grind the fresh petioles of the plant using a meat grinder. Strain the resulting mass through a sieve, leaving the juice. You need to consume it one tablespoon three times a day 30 minutes before meals.
- For the second recipe you will need the root of the plant. It needs to be grated. Then pour two tablespoons of the resulting slurry with 400 ml of boiling water, let it brew and strain. Before each meal, take 50 ml half an hour.
3. Diagnosis of rashes
Idiopathic urticaria can only be diagnosed by an allergist.
.
To do this, he prescribes a series of examinations, the purpose of which is to identify the connection of skin manifestations with specific factors and causes, the elimination of which could prevent the development or exacerbation of urticaria. The patient undergoes the following tests:
- general clinical blood test;
- biochemistry;
- HIV testing;
- blood for the Wasserman reaction;
- general urine analysis;
- blood and feces to identify parasites and helminths.
An important diagnostic step is a conversation with the patient
, during which the possible dependence of skin rashes on food, chemicals, stress, heredity, and medications taken is clarified.
Sometimes it is recommended to keep a symptomatic diary
, where each exacerbation of urticaria is recorded. In this case, the patient should try to remember any previous factors that could affect the state of the body, and also write them down. Sometimes only such records allow us to trace a certain pattern.
If a significant period of careful observation does not give a clear picture, there are no chronic diseases and exacerbations are unsystematic, then a diagnosis of “idiopathic allergy” is made.
About our clinic Chistye Prudy metro station Medintercom page!
Yasnotka
To prepare decoctions, the upper parts of the stem are used during their flowering, since the flowers contain essential oils, tannins, ascorbic acid, and histamine. This composition can cure not only hives, but also other skin diseases.
The decoction will be prepared in a water bath, so you need to prepare two containers in advance. Fill one with water and put on fire, place 2 tablespoons of the dried plant in the second and pour 500 ml of boiling water.
Keep the decoction in a water bath for 20 minutes. Drink half a glass three times a day.
In addition to preparing decoctions for oral administration, yasna also has a local effect. Apply compresses to the blisters that appear or add a decoction to the bath.
Potato
Compresses made from this raw root vegetable have a beneficial effect on blisters that appear, relieving severe itching.
To make such a compress, you must follow the following instructions:
- First, wash and peel the potatoes, then grate them.
- Place the resulting mass on a gauze bandage and apply to the skin area.
- Cover the top of the compress with cling film.
- The duration of the procedure should be no less than half an hour.
- After the time has passed, treat the skin with water at room temperature.
If this type of procedure is intended for children, then its time can be reduced to 15 minutes.
Lotions can be made from potato leaves, as well as other nightshade crops, as they contain a large amount of tannins. They are responsible for relieving swelling and helping the skin calm down.
To prepare, you need to boil a dozen leaves for five minutes, and after cooling, you can begin the procedure. Leave the lotions on for 15 minutes.
What you need to know before starting home treatment
Treatment of urticaria with folk remedies is permissible only after consultation with your doctor. Since in most cases a person with urticaria is prescribed antihistamines, the use of tablets and folk remedies requires caution. The composition of home remedies should not “contradict” medications.
People who think that at home they can get rid of urticaria forever should take into account that urticaria can only be treated symptomatically. Sometimes the disease goes away with age, as happens in children.
If a person visits a doctor, leads a healthy lifestyle, eats right and takes care of his health, he can achieve long-term remission.
Any home remedies are prohibited until it is clear what factors provoke the disease.
General recommendations
Before starting treatment for urticaria, it is necessary to adjust the patient’s lifestyle.
Temporarily give up sports activities. During exercise, the skin sweats and heats up, which provokes even more irritation and pain symptoms. If this is not possible, then immediately after training take a bath with oatmeal.
By rubbing painful areas with ice cubes, you can narrow blood vessels and get rid of swelling and itching. Lotions with camphor oil and menthol eliminate unpleasant burning and itching.
Nettle against allergies
To combat rashes, nettle is used in two forms: added as a decoction to baths and used internally.
Recipes for preparing decoctions for each type:
Place 200 g of dried herb in a saucepan and fill it with three liters of water, keep the decoction on low heat for 15 minutes. After it has cooled, strain through a sieve. Take baths from the decoction for 20 minutes every day for a week.
You need to prepare a decoction for oral administration from 50 grams of dry herb and a glass of water. It is necessary to maintain the heat for half an hour, and after cooling, you can add honey. Before meals you need to drink 100 ml.
In addition, nettle leaves can be used to prepare salads or soups, and can also be added to tea. This will allow the body to get rid of allergic reactions and saturate it with vitamins.
First aid for rashes
A person who is prone to attacks should know what to do with hives if the disease worsens. It is important to learn to recognize the symptoms of anaphylaxis and angioedema, which often accompany urticaria.
A sudden drop in blood pressure, difficulty breathing, hoarseness and pain in the lower abdomen indicate the onset of anaphylactic shock, which requires immediate hospitalization. At the first signs of shock, a person should call an ambulance and take antihistamines, epinephrine (adrenaline), and hormones. These products are prescribed by a doctor and should always be kept in your home medicine cabinet.
- If there are no symptoms of anaphylactic shock, an attack of urticaria is accompanied by rashes and itching, you can limit yourself to an antihistamine, for example, Suprastin or Tavegil.
- It is necessary to immediately remove the allergen that triggered the attack, be it medications or any food, for example, chocolate, wine, citrus fruits.
- If urticaria is a reaction to food, you can take absorbent drugs, activated, white carbon, Enterosgel.
- In case of an insect bite, carefully remove the sting from the skin.
- If the rash is caused by a contact allergen, for example, a cosmetic or detergent, it should be washed off the skin with plenty of warm water.